| World Journal of Nephrology and Urology, ISSN 1927-1239 print, 1927-1247 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Nephrol Urol and Elmer Press Inc |
| Journal website https://wjnu.elmerpub.com |
Original Article
Volume 15, Number 3, July 2026, pages 82-89

Possible Mitigation of Renal Ischemia-Reperfusion Injury With Monk Fruit (Siraitia grosvenori) Extract in a Rat Model
Mohammad Reza Roshandela, Kelvin Zhenga, Andrew Penunuria, Majid Eshghia, Sensuke Konnoa, b ![]()
aDepartment of Urology, New York Medical College, Valhalla, NY 10595, USA
bCorresponding Author: Sensuke Konno, Department of Urology, New York Medical College, Valhalla, NY 10595, USA
Manuscript submitted June 10, 2026, accepted June 29, 2026, published online July 8, 2026
Short title: Mitigation of Renal Injury With Monk Fruit
doi: https://doi.org/10.14740/wjnu1061
| Abstract | ▴Top |
Background: Renal ischemia, induced during various kidney surgeries, alarmingly leads to renal inflammation and injuries. We hypothesized that oxidative stress (OXS) could be a primary cause of renal ischemia-reperfusion injury (RIRI), and that antioxidants may mitigate it. Hence, we investigated if monk fruit extract, LLE, with antioxidant activity might reduce the incidence of warm ischemia-induced RIRI in rats.
Methods: Sprague–Dawley rats were randomly assigned to three groups: (1) Sham, (2) ischemia-reperfusion (RIR), and (3) RIR with LLE supplementation (RIR + LLE). The rat kidney was surgically exposed and subjected to 40-min ischemia by renal pedicle clamping, followed by 24-h reperfusion. LLE (150 μg) was given to rats 30 min prior to ischemia and soon after reperfusion began for 24 h.
Results: The RIR group showed significantly elevated blood urea nitrogen (BUN) and creatinine (Cr) levels, indicating renal dysfunction, and palpable kidney injuries/alterations were also detected by histopathologic examination. However, the kidneys in the RIR + LLE group appeared merely normal with significantly reduced BUN/Cr levels. Additionally, the OXS level was ∼2.3-fold greater, two antioxidant enzymes (catalase and glutathione peroxidase) were inactivated, and specific kidney injury markers (neutrophil-gelatinase-associated lipocalin, kidney injury molecule 1, and clusterin) were up-regulated in the RIR group. In contrast, a few changes in OXS, enzymatic activities, and marker expression were observed in the RIR + LLE group.
Conclusion: This study demonstrates that OXS plays a primary role in RIRI, while LLE with antioxidant activity protects the kidneys from it. Thus, LLE warrants consideration as a potential perioperative renoprotective agent for clinical use.
Keywords: Antioxidant; Ischemia-reperfusion injury; Monk fruit extract; Oxidative stress
| Introduction | ▴Top |
Renal ischemia is commonly induced during nephron-sparing surgery (NSS), renal transplantation, vascular reconstruction, and complex urologic procedures using vascular clamping [1]. Although this clamping minimizes blood loss and allows the surgeon to perform surgery [2], the temporary cessation of renal arterial flow can lead to extensive renal injury, particularly renal ischemia-reperfusion injury (RIRI) [3]. Such RIRI is a primary cause of acute kidney injury (AKI), which is an acute and severe clinical disorder associated with long hospitalization, dialysis dependency, and increased morbidity and mortality [4]. To mitigate RIRI, perioperative strategies are employed during renal surgeries, including dopamine analogs, diuretics, calcium channel blockers, angiotensin-converting enzyme inhibitors, etc. [5, 6]. However, their efficacy remains inconsistent with limited benefits, underscoring the need for more effective renoprotective interventions.
We hypothesized that RIRI is primarily driven by oxidative stress (OXS) [7] because renal ischemia-reperfusion (RIR) induces OXS and inflammation, resulting in structural and functional dysfunction in the kidneys [8, 9]. OXS plays a critical role in the progression of RIRI; however, antioxidants have been reported to be beneficial or therapeutic agents/molecules, capable of reducing or diminishing OXS [10]. Those include vitamins C/E, coenzyme Q10 (CoQ10), reduced glutathione (GSH) etc., which have demonstrated the protective effects against OXS-related cellular damage [11], including RIRI.
We recently came across the bioactive extract of monk fruit (Siraitia grosvenori) [12] (Fig. 1a) whose name is believed to come from an anecdote that Chinese monks have used this fruit as a sweetener for teas or cooking. Its active ingredients are known as “mogrosides,” terpenoid glycosides, having several derivatives (mogroside I–VI) (Fig. 1b). They have a high level of sweetness, i.e., 200–350 times sweeter than sucrose [12], and they have been widely used in commercial dietary products as the US Food and Drug Administration (FDA) considers them to be generally recognized as safe (GRAS) [13].
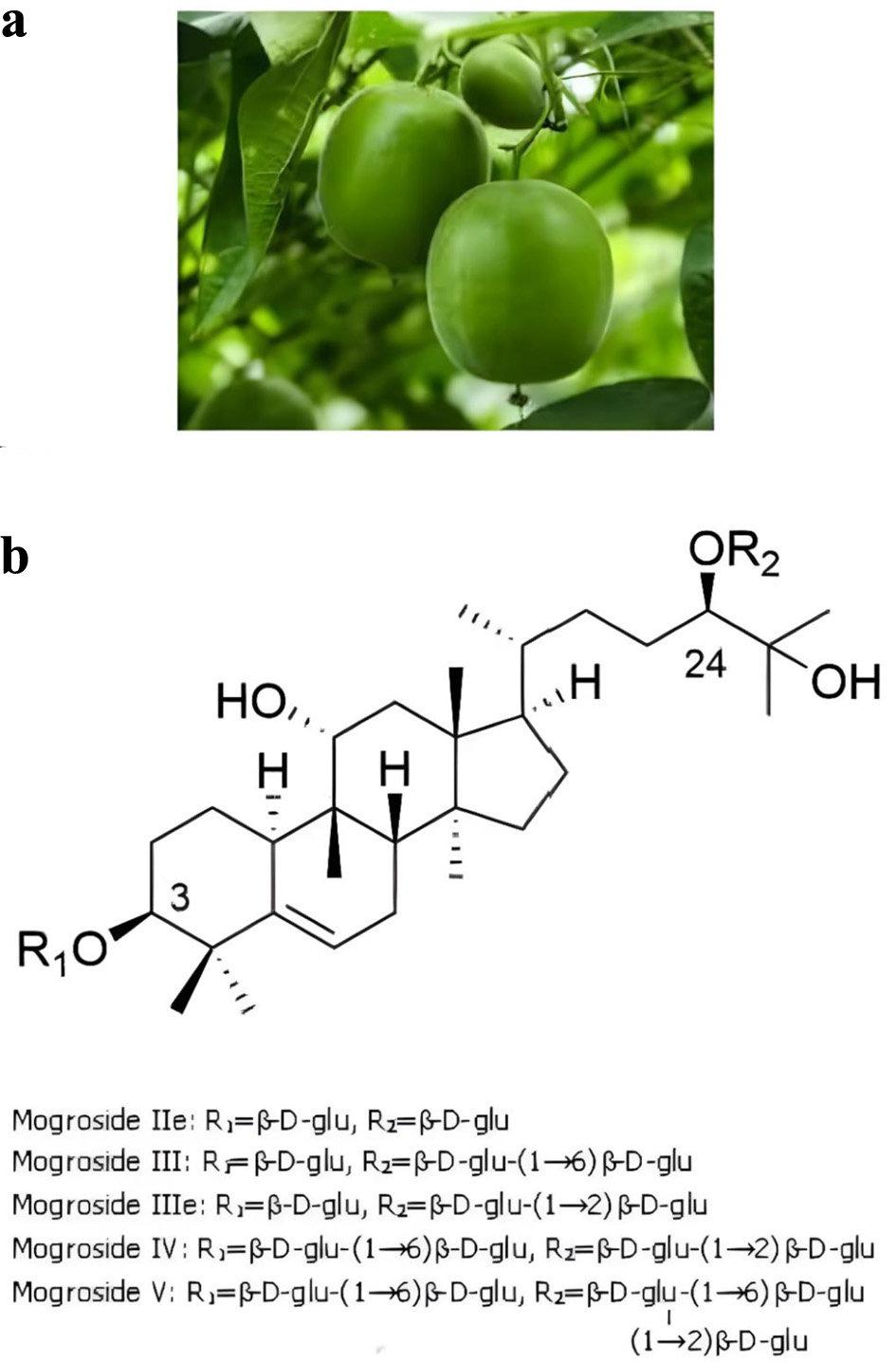 Click for large image | Figure 1. (a) Monk fruit grown on tree. (b) Mogroside derivatives. |
A variety of commercial products of mogrosides were then made and collectively called “Lakanto®” (LKT), exclusively developed by the Japanese company (Saraya Co., Ltd., Osaka, Japan). All LKT products are the proprietary products; however, they have not been fully studied in terms of biological activity besides a natural sweetener. The limited studies have yet revealed their medicinal or pharmacological properties, such as antioxidant, anticancer, anticarcinogenic, anti-diabetic, anti-inflammatory activities, and so forth [12, 14–19]. For instance, their antioxidant activity has been demonstrated in the study of the significant reduction in palmitic acid-induced OXS on pancreatic β cells [17].
Among LKT products, we were particularly interested in LLE with antioxidant activity, which might mitigate OXS-induced RIRI. In this study, LLE was administered orally to rats 30 min prior to ischemia induced by renal pedicle occlusion, as well as immediately after the restoration of reperfusion. Following a 24-h reperfusion period, blood and kidney specimens were collected for evaluating the potential protective effects of LLE. Renal function was assessed by the blood urea nitrogen (BUN)/creatinine (Cr) tests using blood specimens, while kidney specimens (tissues) were used for histopathological examination, severity of OXS, and expressions of RIRI biomarkers. More experimental details and interesting findings are described and discussed herein.
| Materials and Methods | ▴Top |
Cell culture
The porcine renal tubular epithelial LLC-PK1 cells (American Type Culture Collection, Manassas, VA) were employed as our in vitro experimental model. They were maintained in RPMI-1640 medium supplemented with 10% fetal bovine serum (FBS), penicillin (100 units/mL), and streptomycin (100 μg/mL). For experiments, cells were cultured in the six-well plate (2 mL/well) at the initial cell density of 2 × 105 cells/mL and subjected to specific experimental conditions.
Lipid peroxidation (LPO) assay
LLC-PK1 cells were exposed to 70 μM of hydrogen peroxide (H2O2) in the presence or absence of LLE (3 μg/mL) for 3 or 6 h. Cells were then subjected to LPO assay to measure the amount of malondialdehyde (MDA) formed (i.e., severity of OXS) [20]. The detailed procedures are described in the vendor’s protocol (Abcam, Waltham, MA), and the amounts of MDA formed were calculated using the MDA standards and expressed by μM. These μM values obtained were then expressed as the fold increase for a direct comparison.
For rat kidney specimens, approximately 50 mg of kidney tissues was first homogenized and cell extracts were obtained by centrifugation at 4 °C. Fifteen µg of each cell extract were subjected to LPO assay, and the amount of MDA formed was expressed by nmol/mg protein.
Animal study
The procedures used and the care of animals were approved by the Institutional Animal Care and Use Committee (IACUC, #10-2-0216) at New York Medical College (Valhalla, NY). Fifteen Sprague–Dawley rats (∼250 g) were acclimatized for 3 days in a room of the animal facility with controlled temperature (23±2°C), humidity (55±15%), ventilation (15 changes/h), and light (12-h light/dark cycles). They were provided with standard chow and free access to water. Fifteen rats were then randomly divided into the three groups (n = 5 per group): group A (Sham), group B (RIR), and group C (RIR with LLE supplementation (RIR + LLE)).
The warm ischemia-reperfusion experiment essentially followed the procedures described by Cheng at al [21] and Wei et al [22] with minor modifications. One mL of LLE (150 μg/mL) was given to rats through oral gavage 30 min prior to ischemia. After rats were anesthetized, an abdominal midline incision was made and the right kidney was visualized while the left kidney was freed from adjacent perinephric attachments. Ischemia was induced through 40 min of the left renal pedicle occlusion with a microvascular clamp and a blockage of blood flow was confirmed by blue discoloration of the kidney. At the end of the ischemia period (40 min), the clamp was removed and confirmed the blood flow to the kidney (as reperfusion started). After the abdomen was closed, LLE (150 μg) was given through oral gavage and rats were placed in the cage for a 24-h reperfusion interval (the RIR + LLE group). On the other hand, after a removal of the clamp (the end of ischemia), the abdomen of rats (no prior LLE given) was sutured and they were subjected to reperfusion without LLE supplement (the RIR group). In the Sham group, the abdomen was opened and the kidneys were exposed for 40 min without clamping (no ischemia). Following a 40-min interval, the abdomen was closed and rats were placed in the cage.
Assessment of renal function and histopathologic examination of kidney specimens
Following 24-h reperfusion, blood specimens were collected for BUN and Cr analysis, while kidney specimens were surgically excised and subjected to histopathologic examination and biochemical analyses. Both blood and kidney specimens were promptly sent to a commercial pathology laboratory (Antech Diagnostics, New Hyde Park, NY) for analyses. The results of BUN/Cr tests were sent to us, and the pathology report of histopathologic examination, performed by an independent veterinary pathologist, was also sent to us separately.
Assays for antioxidant enzymes
Activities of two key antioxidant enzymes, catalase (CTL) and glutathione peroxidase (GPX) [23], were assessed by CTL and GPX Colorimetric Assay Kit (Catalog Numbers ab83464 and ab102530, respectively). Detailed procedures are described in the manufacture’s protocols (Abcam, Waltham, MA). Briefly, tissue homogenates/extracts were first prepared separately and added to the respective reaction mixtures and incubated at 25 °C for 30 min. The reaction was terminated by adding the Developer mix and incubated at 25 °C for 10 min. All samples were read for CTL at 570 nm or GPX at 340 nm on a microplate reader. All readings were calculated (mU/mL) and CTL and GPX activities were expressed by the % relative to the respective Sham reading (100%).
Western blot analysis
An equal amount (10 μg) of tissue homogenates (obtained from kidney tissues) was first subjected to 10% SDS-polyacrylamide gel electrophoresis and transferred to a nitrocellulose membrane. The blot (membrane) was incubated with primary antibodies against three RIR biomarkers, neutrophil-gelatinase-associated lipocalin (NGAL), kidney injury molecule 1 (Kim-1), and clusterin (CLU) [24] (Santa Cruz Biotechnology, Santa Cruz, CA), for 90 min, followed by 30-min incubation with appropriate secondary antibody conjugates. Specific immunoreactive protein bands were then detected by chemiluminescence following manufacturer’s protocol (Seracare, Milford, MA). Additionally, the density/intensity of those protein bands was quantitated using a scan densitometer (Silk Scientific, Inc., Provo, UT). This analysis was repeated three times to confirm reproducibility, and those densitometric data obtained were then plotted in the graph.
Statistical analysis
All data were presented as mean ± standard deviation (SD), and statistical differences between groups were assessed with either one-way analysis of variance (ANOVA) or the unpaired Student’s t-test. Values of P < 0.05 are considered to indicate statistical significance.
| Results | ▴Top |
Antioxidant effect of LLE (in vitro)
We first examined antioxidant activity of LLE in vitro. Normal kidney LLC-PK1 cells were exposed to H2O2 (70 μM), one of common OXS inducers [25], exerting OXS on cells. The amount of MDA formed was ∼2.5-fold higher in H2O2-treated cells (at 6 h) than that in control cells (Fig. 2), indicating cells under severe OXS. However, such elevated OXS was significantly (25%, P < 0.05) reduced with LLE (Fig. 2), demonstrating its antioxidant activity against H2O2.
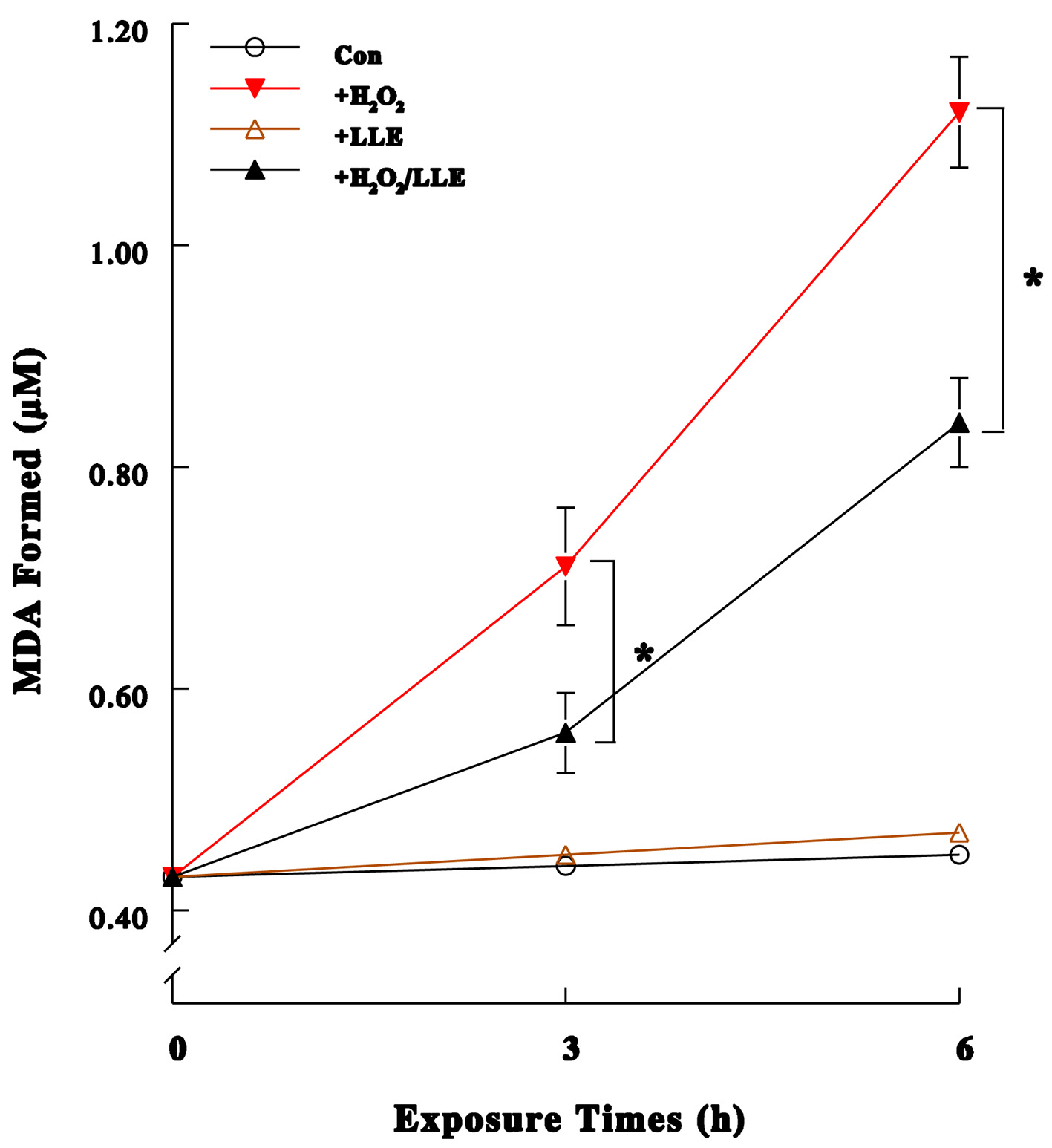 Click for large image | Figure 2. Antioxidant effect of LLE (in vitro). After LLC-PK1 cells were exposed to H2O2 (70 μM) in the presence or absence of LLE (3 μg/mL) for 3 or 6 h, they were subjected to lipid peroxidation (LPO) assay. The amount of malondialdehyde (MDA) formed indicates severity of oxidative stress (OXS) (the greater MDA, the greater OXS). All data are mean ± standard deviation (SD) from three independent experiments (*P < 0.05, H2O2 vs. H2O2/LLE). |
Effects of LLE on renal function following RIR in rats
Once antioxidant activity of LLE was confirmed, whether warm ischemia (RIR)-induced kidney injury would be mitigated with LLE was assessed. Blood analysis showed that the BUN level was a ∼3.7-fold elevated in the RIR group, whereas such an elevated BUN was ∼30% (P < 0.05) decreased with LLE administration (RIR + LLE) (Fig. 3a). Similarly, the Cr level was a ∼2.9-fold higher in the RIR group (than the Sham), but this elevated Cr also ∼27% (P < 0.05) declined with LLE (Fig. 3b). Thus, LLE appears to significantly (P < 0.05) prevent/reduce the loss of renal function (dysfunction) caused by RIR.
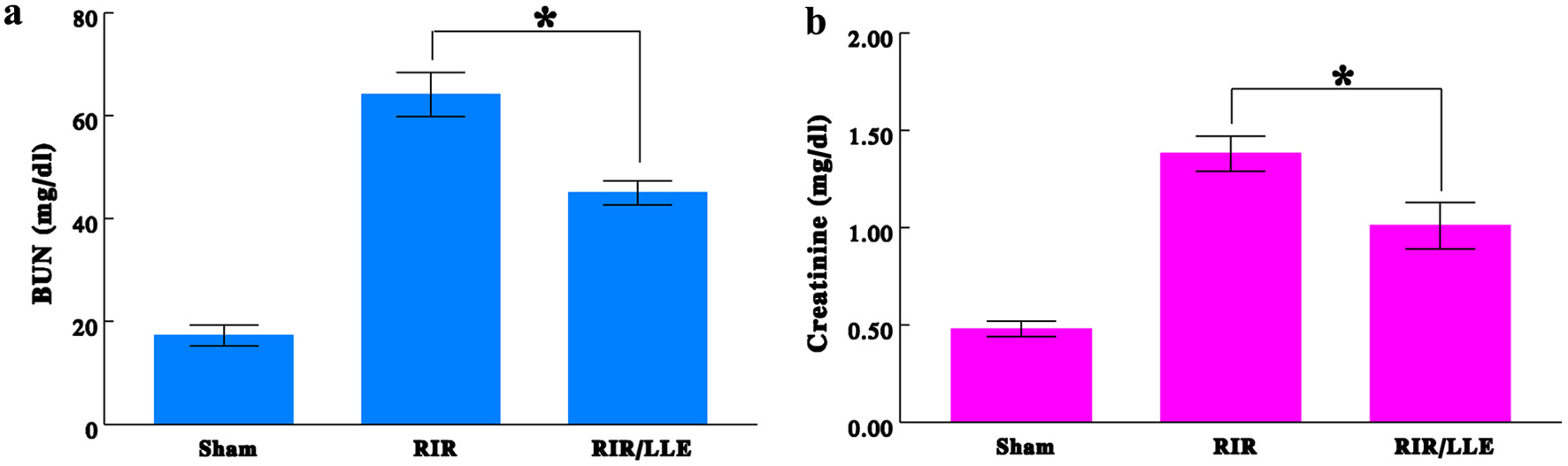 Click for large image | Figure 3. Effects of renal ischemia-reperfusion (RIR) and RIR/LLE on blood urea nitrogen (BUN) and creatinine. Blood specimens collected from the rats were analyzed for the BUN (a) and creatinine (b) levels. The data are mean ± standard deviation (SD) from three samples of each group (*P < 0.05, RIR vs. RIR/LLE). |
Histopathologic examination on rat kidneys
Histopathologic examination of kidney tissues revealed that tubular degeneration was predominantly found in the corticomedullary junction (CMJ) region in the kidney of RIR rats. These tubules were lined by epithelial cells of varying size with enlarged and flattened cells (Fig. 4b), exhibiting morphological alterations. In contrast, LLE-given rats under RIR (RIR + LLE) showed less histological changes (Fig. 4c), nearly similar to the Sham group (Fig. 4a). Therefore, these results demonstrate that LLE is capable of mitigating RIRI during the RIR period.
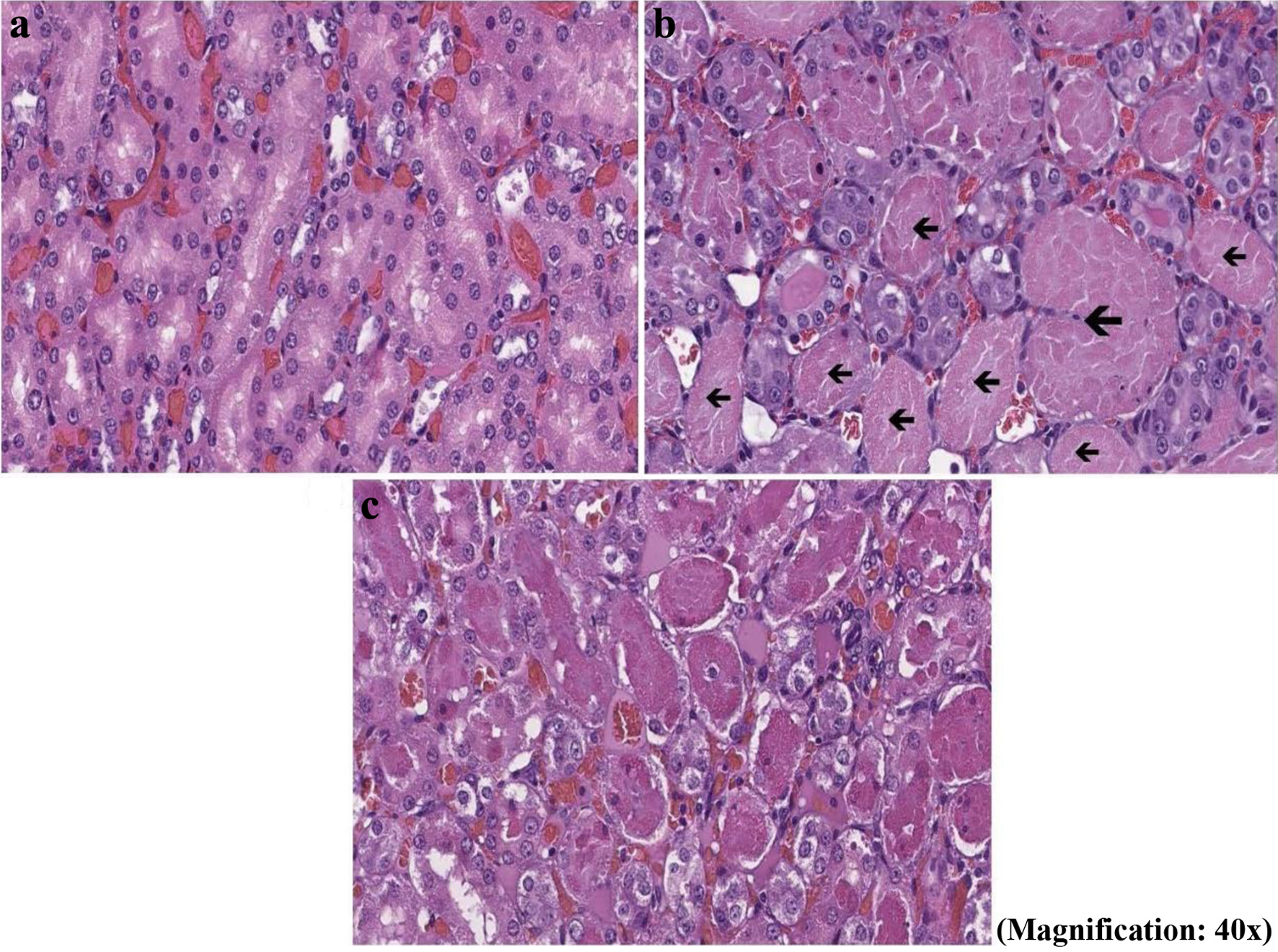 Click for large image | Figure 4. Histopathologic examination of kidney tissues. The corticomedullary junction (CMJ) regions of kidney tissues obtained from three different experimental conditions—Sham (a), renal ischemia-reperfusion (RIR) (b), and RIR + LLE (c)—were histopathologically examined and photographed. Hematoxylin & eosin (H&E) staining showed enlarged and flattened tubular cells indicated by black arrows. |
Exertion of RIR-induced OXS on kidney specimens
We next performed LPO assay on rat kidney tissues to assess the severity of OXS exerted on the kidney during RIR procedures. The amount of MDA formed in the rat kidney under RIR was a ∼2.3-fold greater than that in the Sham group (Fig. 5a). However, such severe OXS was ∼42% (P < 0.05) diminished with LLE administration (RIR + LLE) (Fig. 5a). Thus, RIR-induced OXS could be significantly reduced or diminished with LLE owing to its antioxidant activity.
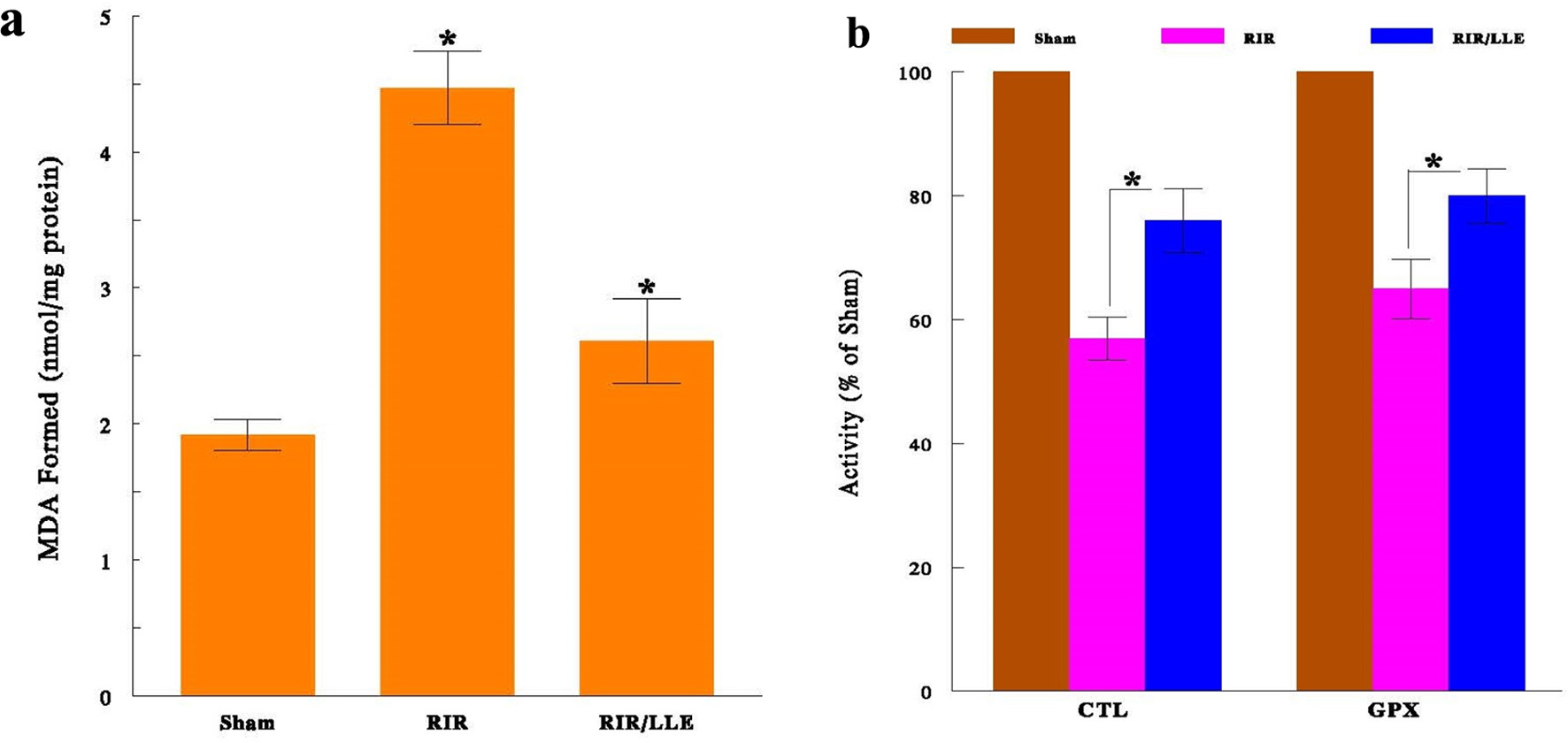 Click for large image | Figure 5. (a) Oxidative stress (OXS) on kidneys during renal ischemia-reperfusion (RIR). OXS in different experimental conditions was assessed in kidney tissues by lipid peroxidation (LPO) assay. All data are mean ± standard deviation (SD) from three individual specimens of each experimental group (*P < 0.05 compared with Shams). (b) Inactivation of antioxidant enzymes during RIR. Three different experimental conditions of kidney tissues were assayed for activities of two antioxidant enzymes, catalase (CTL) and glutathione peroxidase (GPX). The data are mean ± standard deviation (SD) from three specimens of each group (*P < 0.05, RIR vs. RIR/LLE). |
Inactivation of antioxidant enzymes in rat kidneys
We also wondered whether such severely induced OXS might have come from another factor, such as an adverse effect on antioxidant enzymes [23], which play a major defense role against OXS. Activities of two key antioxidant enzymes, CTL and GPX, were then assessed. The results showed that CTL and GPX activities declined to ∼57% and ∼65% during the RIR period, respectively (Fig. 5b). However, LLE significantly protected them with sustaining nearly 80% of their activities (Fig. 5b). Thus, inactivation of these enzymes by RIR may account for even more severe OXS.
Effects of RIR on RIRI biomarkers
Whether RIR would adversely affect the kidney at the molecular level was also assessed. Three specific biomarkers of renal cell injury, NGAL, Kim-1, and CLU [24], were examined using Western blot analysis. Such analysis revealed that the expressions of three markers were all up-regulated or elevated under RIR (the RIR group), compared with those in the Sham group (Fig. 6a). Actually, densitometric analysis, quantitating the density of protein bands/expressions in these markers, showed over fivefold greater in the RIR group than that in the Sham group (Fig. 6b). However, those rats receiving LLE under RIR (RIR + LLE) showed no such enhanced expressions, nearly similar to those in the Sham (Fig. 6a, b). Thus, these findings suggest that the rat kidney under RIR corroborates extensive renal cell injury (RIRI) at the molecular level, evidenced by the up-regulation (enhanced expressions) of these markers [24]. Nonetheless, LLE significantly protected the kidney from such injury as all markers remained intact (RIR + LLE), demonstrating the renoprotective effect of LLE against OXS.
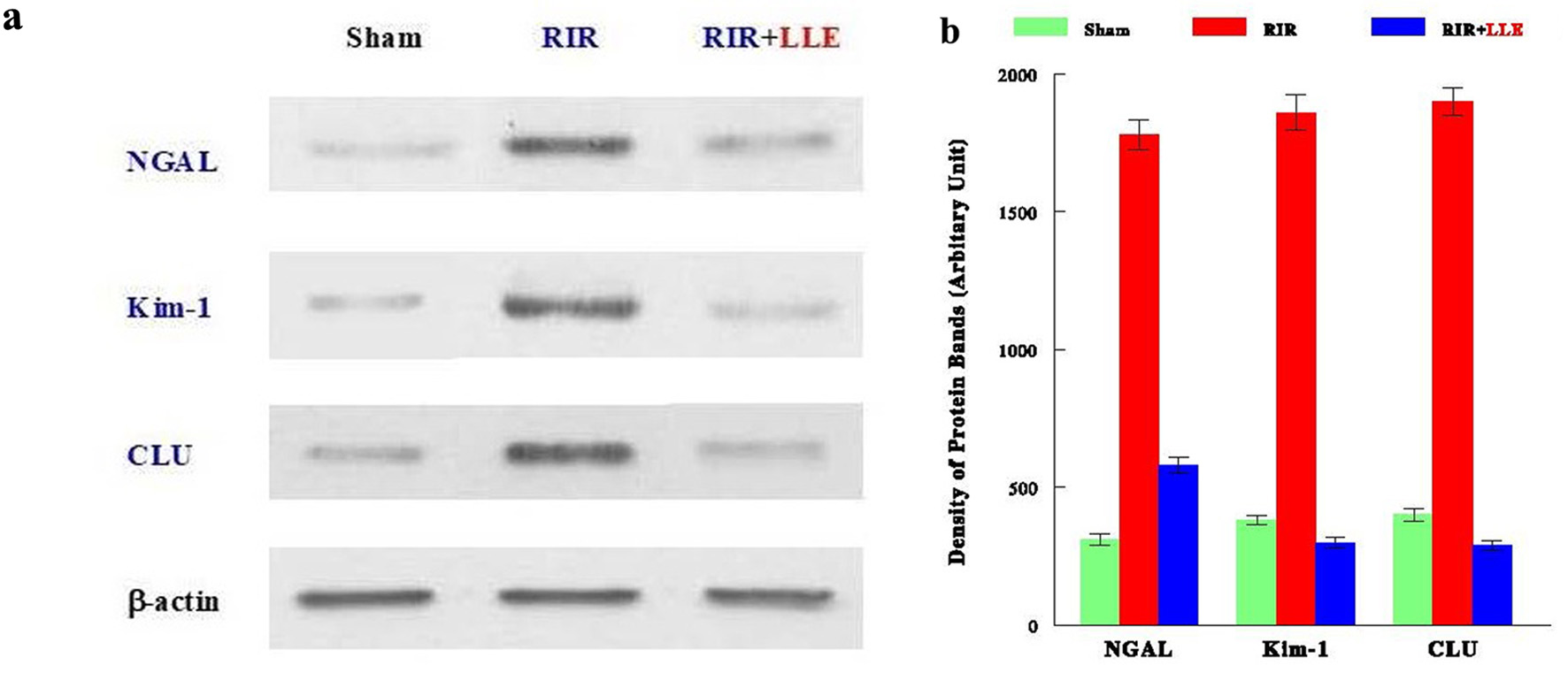 Click for large image | Figure 6. Up-regulation of renal ischemia-reperfusion injury (RIRI) biomarkers under renal ischemia-reperfusion (RIR). Kidney tissues from three experimental conditions were analyzed for three RIRI biomarkers (NGAL, Kim-1 and CLU) using Western blots. (a) Autoradiographs of these markers are shown and β-actin was also run as a protein loading control. (b) The density of the protein bands was also quantified by scan densitometry and plotted in the graph. |
| Discussion | ▴Top |
We have explored the potential role of LLE in preserving renal function during ischemia induced in renovascular surgeries using a rat model. Ischemia was induced by 40 min of vascular clamping, followed by 24-h reperfusion in rats. The oxygen and nutrient supply to renal tubular cells will be impaired during ischemia, but reperfusion usually restores blood flow. Nevertheless, glomerular, vascular, and tubular disturbances would remain and even exacerbate to cause RIRI during the reperfusion period [26], eventually resulting in AKI and renal dysfunction [3]. Thus, it is imperative to establish strategies to mitigate renal injury, preserving renal function. We then investigated if LLE with antioxidant activity [12] could effectively mitigate/alleviate RIRI in rats because of OXS being a causal factor for RIRI. LLE was chosen because we were always interested in using natural products in our research, due to few side effects [27].
We first examined antioxidant activity of LLE in vitro by placing normal kidney LLC-PK1 cells under H2O2-induced OXS in the presence/absence of LLE. LPO assay showed that severe OXS induced by H2O2 was significantly diminished with LLE, demonstrating antioxidant activity of LLE (against H2O2).
We then proceeded the study of LLE effects on warm ischemia-induced rats. A loss of kidney function (dysfunction) was evidenced by the significant increase in the BUN and Cr levels during the RIR period. However, such elevated BUN/Cr levels were significantly reduced with LLE supplement (RIR/LLE).
Histopathologic examination was specifically performed on the CMJ region of the kidney because it is the region where RIRI predominantly occurs [28]. After ischemia, although renal blood flow usually becomes normal (in the cortex and medulla regions) during reperfusion, it yet remains merely 10% of normal in the CMJ area, due to the microvascular congestion. It is thus plausible that such reduced blood flow for 24 h during reperfusion would worsen renal function and facilitate pathological alterations [29]. Our study revealed histomorphological alterations (tubular degeneration, cellular enlargement, intratubular casts, etc.) in the CMJ region following RIR. However, those rats supplemented with LLE during RIR (RIR + LLE) showed minimal changes in their kidneys. Thus, LLE may effectively protect the rat kidneys from RIR, mitigating subsequent RIRI and minimizing pathological changes.
LLE appears to effectively prevent or mitigate RIRI when RIR is exerted. It is more likely attributed to its antioxidant activity, diminishing OXS induced by RIR. This confirms that OXS is a major factor causing the various and serious outcomes of RIR.
Hence, antioxidant activity of LLE is rather significant, and another study of mogrosides [12], active ingredients of LLE, demonstrated such antioxidant activity in pancreatic β cells [17]. As briefly mentioned earlier, pancreatic β cells are vulnerable to OXS, due to low antioxidant activity, and especially a high level of palmitic acid present in the microenvironment is an inevitable threat of OXS. In fact, palmitic acid can cross the cellular membrane and enter mitochondria where OXS is generated and exerts, resulting in severe β-cell damage. However, mogrosides were found to significantly reduce such OXS, protecting and sustaining normal β-cell function. Thus, mogrosides with potent antioxidant activity, diminishing palmitic acid-induced OXS in pancreatic β cells, would restore normal insulin secretion function to prevent the development and progression of diabetes.
Besides LLE or mogrosides, pomegranate extract (PE) is another natural extract, which has been reported to effectively protect the rat kidneys from RIRI [10]. It is similar to our study, in which rats were subjected to RIR but PE ameliorated the oxidative damage (by OXS) and histopathological changes following RIR. PE is known to have polyphenol antioxidants (tannins and anthocyanins) and was also used to treat some diseases. Like LLE, as PE has little side effects to be concerned, it could be safely and effectively used to protect the (human) kidneys from RIRI.
Additionally, fimasartan (angiotensin receptor antagonist) is a drug that has been shown to ameliorate RIRI in rats [8]. This drug was capable of protecting the rat kidneys from RIRI through modulation of OXS, the inflammatory cascade, and apoptotic effect. As a result, normal renal function was stored and cell morphology also remained nearly normal. Since fimasartan is shown to have a safety profile, efficacy, and tolerability, it could be clinically used as the protective agent for RIRI.
Now, we wondered if such profound OXS-mediated outcomes following RIR were due solely to the severity of OXS itself, not to some other factor(s). We then found that OXS also led to inactivation of two antioxidant enzymes, CTL and GPX. This finding is significant because it implies that RIR exerts OXS, which also inactivates antioxidant enzymes. Hence, it is rather possible that even severer OXS (due to inactivation of enzymes) could be exerted on the kidneys under RIR, leading to such extensive alterations in renal function and cell morphology. However, those renal changes (including enzyme inactivation) were significantly mitigated/reduced with LLE supplement. Moreover, it is plausible that various renal diseases/disorders, due to renal cell injury, would be somehow linked to the certain degrees of OXS.
Lastly, RIRI is known to have adverse effects on renal cells at the cellular/pathological level [30], but it can also affect them at the molecular level. We showed that three RIRI markers (NGAL, Kim-1, and CLU) [24] were all up-regulated under RIR, confirming positive RIRI at the molecular level as well. However, such molecular changes were effectively prevented with LLE.
Conclusion
The present study demonstrates that oxidative stress, induced during a warm ischemia-reperfusion period, would play a crucial role in acute renal injury (RIRI). Nevertheless, LLE with antioxidant activity was capable of effectively mitigating RIRI-induced renal dysfunction, altered cell morphology, and inactivation of antioxidant enzymes in rats. As these findings are encouraging and promising, LLE may serve as a perioperative agent, offering its potential therapeutic benefits during renal surgeries. Further investigations are thus warranted to validate the applicability of LLE in clinical settings.
Acknowledgments
We gratefully acknowledge Saraya Co., Ltd. (Osaka, Japan) for the generous gift of LLE used in this study.
Financial Disclosure
None to declare.
Conflict of Interest
The authors have nothing to disclose.
Informed Consent
Not applicable.
Author Contributions
MRR: methodology and investigation; KZ: investigation and software; AP: investigation and data curation; ME: resources and supervision; SK: conceptualization, validation, writing – original draft.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Mir MC, Pavan N, Parekh DJ. Current paradigm for ischemia in kidney surgery. J Urol. 2016;195(6):1655-1663.
doi pubmed - Desai MM, de Castro Abreu AL, Leslie S, Cai J, Huang EY, Lewandowski PM, Lee D, et al. Robotic partial nephrectomy with superselective versus main artery clamping: a retrospective comparison. Eur Urol. 2014;66(4):713-719.
doi pubmed - Malek M, Nematbakhsh M. Renal ischemia/reperfusion injury; from pathophysiology to treatment. J Renal Inj Prev. 2015;4(2):20-27.
doi pubmed - Loef BG, Henning RH, Navis G, Rankin AJ, van Oeveren W, Ebels T, Epema AH. Changes in glomerular filtration rate after cardiac surgery with cardiopulmonary bypass in patients with mild preoperative renal dysfunction. Br J Anaesth. 2008;100(6):759-764.
doi pubmed - Zacharias M, Mugawar M, Herbison GP, Walker RJ, Hovhannisyan K, Sivalingam P, Conlon NP. Interventions for protecting renal function in the perioperative period. Cochrane Database Syst Rev. 2013;2013(9):CD003590.
doi pubmed - Conger JD. Interventions in clinical acute renal failure: what are the data? Am J Kidney Dis. 1995;26(4):565-576.
doi pubmed - Baliga R, Ueda N, Walker PD, Shah SV. Oxidant mechanisms in toxic acute renal failure. Am J Kidney Dis. 1997;29(3):465-477.
doi pubmed - Abbas W, Altemimi M, Qassam H, Hameed AA, Zigam Q, Abbas L, Jabir M, et al. Fimasartan ameliorates renal ischemia reperfusion injury via modulation of oxidative stress, inflammatory and apoptotic cascades in a rat model. J Med Life. 2022;15(2):241-251.
doi pubmed - Hashemi SS, Janfeshan S, Karimi Z. Acute lung injury induced by acute uremia and renal ischemic-reperfusion injury: The role of toll-like receptors 2 and 4, and oxidative stress. Iran J Basic Med Sci. 2022;25(5):643-651.
doi pubmed - Sancaktutar AA, Bodakci MN, Hatipoglu NK, Soylemez H, Basarili K, Turkcu G. The protective effects of pomegranate extracts against renal ischemia-reperfusion injury in male rats. Urol Ann. 2014;6(1):46-50.
doi pubmed - Cutler RG. Antioxidants and aging. Am J Clin Nutr. 1991;53(1 Suppl):373S-379S.
doi pubmed - Li C, Lin LM, Sui F, Wang ZM, Huo HR, Dai L, Jiang TL. Chemistry and pharmacology of Siraitia grosvenorii: a review. Chin J Nat Med. 2014;12(2):89-102.
doi pubmed - U.S. Food and Drug Administration. GRAS Notice 000706: Siraitia grosvenorii Swingle (Luo Han Guo) Fruit Extracts 2018. https://www.fda.gov/media/109982/download.
- Yasuno H, Nishimura J, Dewa Y, Muguruma M, Takabatake M, Murata Y, Shibutani M, et al. Modifying effect of Siraitia grosvenori extract on piperonyl butoxide-promoted hepatocarcinogenesis in rats. J Toxicol Sci. 2008;33(2):197-207.
doi pubmed - Takasaki M, Konoshima T, Murata Y, Sugiura M, Nishino H, Tokuda H, Matsumoto K, et al. Anticarcinogenic activity of natural sweeteners, cucurbitane glycosides, from Momordica grosvenori. Cancer Lett. 2003;198(1):37-42.
doi pubmed - Takeo E, Yoshida H, Tada N, Shingu T, Matsuura H, Murata Y, Yoshikawa S, et al. Sweet elements of Siraitia grosvenori inhibit oxidative modification of low-density lipoprotein. J Atheroscler Thromb. 2002;9(2):114-120.
doi pubmed - Xu Q, Chen SY, Deng LD, Feng LP, Huang LZ, Yu RR. Antioxidant effect of mogrosides against oxidative stress induced by palmitic acid in mouse insulinoma NIT-1 cells. Braz J Med Biol Res. 2013;46(11):949-955.
doi pubmed - Suzuki YA, Tomoda M, Murata Y, Inui H, Sugiura M, Nakano Y. Antidiabetic effect of long-term supplementation with Siraitia grosvenori on the spontaneously diabetic Goto-Kakizaki rat. Br J Nutr. 2007;97(4):770-775.
doi pubmed - Di R, Huang MT, Ho CT. Anti-inflammatory activities of mogrosides from Momordica grosvenori in murine macrophages and a murine ear edema model. J Agric Food Chem. 2011;59(13):7474-7481.
doi pubmed - Dargel R. Lipid peroxidation—a common pathogenetic mechanism? Exp Toxicol Pathol. 1992;44(4):169-181.
doi pubmed - Cheng YT, Tu YC, Chou YH, Lai CF. Protocol for renal ischemia-reperfusion injury by flank incisions in mice. STAR Protoc. 2022;3(4):101678.
doi pubmed - Wei Q, Dong Z. Mouse model of ischemic acute kidney injury: technical notes and tricks. Am J Physiol Renal Physiol. 2012;303(11):F1487-1494.
doi pubmed - Wieczorek E, Jablonowski Z, Tomasik B, Gromadzinska J, Jablonska E, Konecki T, Fendler W, et al. Different gene expression and activity pattern of antioxidant enzymes in bladder cancer. Anticancer Res. 2017;37(2):841-848.
doi pubmed - Charlton JR, Portilla D, Okusa MD. A basic science view of acute kidney injury biomarkers. Nephrol Dial Transplant. 2014;29(7):1301-1311.
doi pubmed - Liou GY, Storz P. Reactive oxygen species in cancer. Free Radic Res. 2010;44(5):479-496.
doi pubmed - Karimi Z, Asadi K, Ghahramani P, Gholami A. Trinitroglycerine-loaded chitosan nanoparticles attenuate renal ischemia-reperfusion injury by modulating oxidative stress. Sci Rep. 2024;14(1):32112.
doi pubmed - Gupta C, Prakash D. Phytonutrients as therapeutic agents. J Complement Integr Med. 2014;11(3):151-169.
doi pubmed - Molitoris BA, Sandoval R, Sutton TA. Endothelial injury and dysfunction in ischemic acute renal failure. Crit Care Med. 2002;30(5 Suppl):S235-240.
doi pubmed - Biology of acute renal failure: therapeutic implications. Kidney Int. 1997;52(4):1102-1115.
doi pubmed - Padanilam BJ. Cell death induced by acute renal injury: a perspective on the contributions of apoptosis and necrosis. Am J Physiol Renal Physiol. 2003;284(4):F608-627.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
World Journal of Nephrology and Urology is published by Elmer Press Inc.