| World Journal of Nephrology and Urology, ISSN 1927-1239 print, 1927-1247 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Nephrol Urol and Elmer Press Inc |
| Journal website https://wjnu.elmerpub.com |
Original Article
Volume 15, Number 3, July 2026, pages 71-81

Association Between Bladder Volume Changes and Organ-at-Risk Dose Constraints in a Moderate Hypofractionation for Prostate Cancer
Natcha Senawina, Suppadech Tunruttanakulb, d ![]() , Sorathan Chanjorahkea, Phruetiporn Thainsitiporna, Sasiprapa Niamsawana, Jayanton Patumanondc
, Sorathan Chanjorahkea, Phruetiporn Thainsitiporna, Sasiprapa Niamsawana, Jayanton Patumanondc
aDivision of Radiation Oncology, Department of Radiology, Sawanpracharak Hospital, Nakhon Sawan 60000, Thailand
bDivision of Innovation and Research, Regional Health Promotion Center 3, Nakhon Sawan, Thailand
cClinical Epidemiology Unit, Faculty of Medicine, Naresuan University, Phitsanulok, Thailand
dCorresponding Author: Suppadech Tunruttanakul, Division of Innovation and Research, Regional Health Promotion Center 3, Nakhon Sawan 60000, Thailand
Manuscript submitted March 11, 2026, accepted June 4, 2026, published online July 8, 2026
Short title: Bladder Volume and OAR Dose in Prostate RT
doi: https://doi.org/10.14740/wjnu1056
| Abstract | ▴Top |
Background: The aim of the study was to evaluate the association between bladder volume and dose-volume constraints of organs at risk—specifically the bladder and rectum—in patients receiving moderately hypofractionated radiotherapy for localized prostate cancer, and to identify factors associated with exceeding organs-at-risk dose constraints.
Methods: This retrospective study included patients who received either 70 Gy in 28 fractions or 60 Gy in 20 fractions using volumetric modulated arc therapy with daily cone beam computed tomography. Bladder volume was measured at each session. Multilevel mixed-effects linear regression was used to assess the association between bladder volume and organs-at-risk dose constraints. Zero-inflated Poisson regression was applied to explore factors associated with organs-at-risk dose overdose, defined according to the Radiation Therapy Oncology Group (RTOG) 0415 and Conventional or Hypofractionated High Dose Intensity Modulated Radiotherapy in Prostate Cancer (CHHiP) trial thresholds.
Results: A total of 388 radiotherapy sessions were analyzed among 15 patients. Increased bladder volume was significantly associated with reduced radiation exposure to organs at risk. This protective effect was more pronounced for the urinary bladder (risk difference: −6.4% to −7.8% per 100 mL increase) than for the rectum (−1.0% to −2.2%) under the 70 Gy protocol. No significant rectal protection was observed under the 60 Gy protocol. The 60 Gy protocol (risk ratio = 15.4; 95% confidence interval, 2.93–81.02) and high recurrence risk (risk ratio = 2.41; 95% confidence interval, 1.12–5.16) were significant predictors of bladder overdose. The 60 Gy protocol was the only significant predictor of rectal overdose.
Conclusions: Larger bladder volumes reduce radiation exposure to organs at risk, particularly the urinary bladder. Rectal protection was limited, especially under the 60 Gy protocol. Optimizing bladder volume may improve treatment safety and adherence to dose constraints.
Keywords: Prostate cancer; Radiation dose hypofractionation; Volumetric modulated arc therapy; Organs at risk; Retrospective study
| Introduction | ▴Top |
Prostate cancer is the second most common cancer in men. Moderate hypofractionated radiotherapy regimens are commonly offered for localized prostate cancer [1, 2]. Moderate hypofractionation delivers a higher dose per fraction (2.4–4.0 Gy) compared to conventional fractionation (1.8–2.0 Gy). Several studies have shown that cancer control outcomes and late toxicity of moderately hypofractionated radiotherapy are similar to conventional radiotherapy. The main advantage of moderate hypofractionation is a shorter treatment duration of 4–6 weeks, compared to 7–8 weeks with conventional fractionation [1, 2].
Volumetric modulated arc therapy (VMAT) allows for high-dose conformity to the tumor while minimizing the dose to surrounding normal tissue. However, variations in bladder volume during daily treatment can impact dosimetry in organs at risk (OARs) [3–5]. In VMAT treatment planning, dose limitations are set for the bladder (genitourinary (GU)) and rectum (gastrointestinal (GI)). GU and GI toxicity are significant concerns in external beam radiotherapy (EBRT). Cone beam computed tomography (CBCT) provides image guidance that helps assess bladder volume and minimize OAR toxicities.
Although several studies have reported associations between bladder volume and dose to OARs [3–5], prior analyses have often been limited to comparisons between predefined bladder-filling states or single time-point assessments. More recent studies have also explored dosimetric variation using daily imaging and motion analysis [6, 7]. The relationship between bladder volume and dose–volume constraint behavior across repeated treatment sessions within the same patients, analyzed using session-level data and accounting for within-patient variability, has been explored in prior studies using different methodological approaches, particularly with respect to study design and analytical strategies [8, 9]. Moreover, the evidence regarding rectum as an OAR remains inconclusive, with prior studies showing inconsistent or limited associations [9, 10]. The aim of this study was to evaluate the association between bladder volume changes and OAR dose constraints under a moderate hypofractionated radiotherapy protocol, while accounting for repeated measures in individual patients. A secondary aim was to identify risk factors associated with exceeding OAR dose constraints in this treatment setting.
| Materials and Methods | ▴Top |
This study was a retrospective observational cohort study. We included patients with histologically confirmed localized prostate cancer, who received moderate hypofractionated radiotherapy using VMAT planning. Two treatment protocols were used: 70 Gy in 28 fractions (2.5 Gy per fraction) and 60 Gy in 20 fractions (3 Gy per fraction). The treatment protocol was selected by the attending radiation oncologist after discussion with the patient. The recruitment period was from May 2022 to April 2024. The study setting (Sawanpracharak Hospital) was a tertiary government hospital in Thailand’s Region 3 health care area. This healthcare area, during the study period, had only one radiotherapy facility, which was located in the study setting. We excluded patients with metastatic prostate cancer, bladder or rectal invasion, and those who did not undergo daily CBCT image guidance. All data were retrieved from the hospital electronic archiving system and the Eclipse Treatment Planning System, version 16.0.
Our department had a bowel and urinary bladder preparation protocol for all patients. After emptying their rectum and bladder, patients drank 600 mL of water within 10–15 min and waited for 40–75 min before computed tomography (CT) simulation and then received daily treatment. For VMAT planning, the clinical target volume (CTV), planning target volume (PTV), and OARs (the bladder and rectum) were delineated on the CT planning images by the radiation oncologists. The PTV was defined according to institutional protocols, which may include seminal vesicles in patients with higher-risk disease, depending on clinical indications. Treatment planning followed fractionation and dose-volume constraints for both target volumes and OARs, adhering to the Radiation Therapy Oncology Group (RTOG) 0415 and Conventional or Hypofractionated High Dose Intensity Modulated Radiotherapy in Prostate Cancer (CHHiP) trial protocols for 70 Gy and 60 Gy, respectively [11, 12].
Assessment of dose-volume histograms (DVHs), CT simulation plans, and daily pre-treatment CBCT images was performed using the Eclipse Treatment Planning System, version 16.0. Bladder volume (mL) was measured on each daily CBCT image, and DVH data for both the bladder and rectum were recorded.
During treatment, CBCT was used for image guidance to verify patient positioning before treatment delivery. Pre-treatment CBCT was acquired to confirm the target volume and OARs. The bladder and rectum were delineated on the daily CBCT images for each patient by the radiation oncologist. CBCT images were used solely for re-delineation of the bladder and rectum to assess daily organ volume and morphological variation. The newly contoured OAR structures were transferred to the planning CT via rigid image registration between the daily CBCT and the planning CT images. The original planning CT–based dose matrix was preserved and applied to the transferred OAR contours for each fraction. DVH parameters were then extracted from the original dose distribution using the updated bladder and rectum structures. No dose recalculation was performed on the CBCT datasets. This approach assumes that the planned dose distribution remains unchanged across fractions and does not account for variations in tissue density or deformation-related dose redistribution.
Dose-volume constraints for OARs, expressed as the percentage of organ volume receiving specific radiation doses, were derived from DVH data. For the 70 Gy in 28 fractions protocol, dose-volume constraints based on RTOG 0415 were applied, including bladder constraints of V79 < 15%, V74 < 25%, V69 < 35%, and V50 < 50%, and rectal constraints of V74 < 15%, V69 < 25%, V64 < 35%, and V50 < 50%, where Vx represents the percentage of the organ volume receiving a radiation dose of at least x Gy. For the 60 Gy in 20 fractions protocol, based on the CHHiP trial, bladder constraints included V60 < 5%, V48.6 < 25%, and V40.8 < 50%, while rectal constraints were V60 < 3%, V57 < 15%, V52.8 < 30%, V48.6 < 50%, and V40.8 < 60%. In brief, under the 70-Gy protocol, the dose-volume constraint V79 < 15% for the bladder indicates that no more than 15% of the bladder volume should receive 79 Gy.
We treated bladder and rectum dose constraints as the dependent (outcome) variables. Bladder volume (mL) was our main examined factor and was calculated from the daily pre-treatment CBCT images for every radiation session. Other collected factors that could affect OAR overdose were patients’ age, unfavorable or high prostate cancer recurrence risk, bladder filling time, and radiation protocol (70 Gy or 60 Gy). Risk groups were determined according to the National Comprehensive Cancer Network (NCCN) classification.
To assess clinical relevance, all patients were evaluated 1 year after completing radiotherapy to determine the occurrence of radiation-induced urinary or rectal complications, which were classified as acute (< 90 days) or chronic (≥ 90 days) [13]. Toxicity was also graded according to the Radiation Therapy Oncology Group (RTOG) criteria.
The study protocol was approved by the Sawanpracharak Hospital Ethical Committee for Research in Human Subjects (COA.7/2023). This study was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki Declaration. All participants remained anonymous, and no identifiable individual data were used in the analysis.
Statistical analysis
Continuous variables were summarized as mean ± standard deviation, and discrete variables as counts and percentages.
Because each participant received multiple treatment sessions with repeated parameter measurements, analyses were performed using multilevel mixed-effects models. According to our main objective (assessing the relationship between OAR constraints and bladder volume), we analyzed the association using multilevel mixed-effects linear regression [8]. The OAR constraints were the main dependent variables, and bladder volume measured at each session was the key independent variable. Individual patients were included as random effects in the model. Age, unfavorable/high prostate cancer recurrence risk, and bladder filling time were included as adjusted independent variables. Given the limited number of patients, the number of covariates included in the multivariable models was intentionally restricted to avoid overfitting, and variables were selected based on clinical relevance. Graphical associations between bladder volume and OAR dose constraints were generated.
Our secondary objective was to assess factors affecting OAR overdose. The main outcomes, bladder and rectum constraints, were further categorized according to whether the urinary bladder or rectum received a higher percentage volume than the specified radiation dose thresholds during individual sessions (based on the RTOG 0415 and CHHiP trial criteria). For the 70-Gy protocol, over-volume bladder constraints were V79 ≥ 15%, V74 ≥ 25%, V69 ≥ 35%, and V50 ≥ 50%, and over-volume rectal constraints were V74 ≥ 15%, V69 ≥ 25%, V64 ≥ 35%, and V50 ≥ 50%. For the 60-Gy protocol, over-volume bladder constraints were V60 ≥ 5%, V48.6 ≥ 25%, and V40.8 ≥ 50%, and over-volume rectal constraints were V60 ≥ 3%, V57 ≥ 15%, V52.8 ≥ 30%, V48.6 ≥ 50%, and V40.8 ≥ 60%.
Because each over-volume constraint represents a different level of clinical severity, we constructed a weighted count of overdose events per session by assigning weights based on the relative importance of each constraint threshold (e.g., for the 70-Gy bladder protocol, V79 (more serious) was weighted as 1−0.15 = 0.85, while V50 (less serious) was weighted as 1−0.50 = 0.50). This resulted in a composite outcome reflecting both the frequency and relative severity of constraint violations.
Although the weighting scheme may yield non-integer values, the outcome retains a count-based interpretation at the session level. To account for the high proportion of sessions without overdose events, a zero-inflated Poisson model was applied [14], with a constant inflation term to model excess zeros. The count component included session number as a linear term, and a random effect for individual patients was incorporated to account for repeated measurements. Examined factors included bladder volume, patient age, unfavorable/high prostate cancer recurrence risk, bladder filling time, and radiation protocol (70 vs. 60 Gy).
We calculated the sample size based on a pilot study of five patients (four receiving the 70-Gy protocol and one receiving the 60-Gy protocol). The pilot analysis included all available CBCT-guided treatment sessions from the five patients, with each patient contributing multiple fractions (total of 137 sessions). Given the small and imbalanced sample, the pilot study was intended only to provide preliminary estimates of effect size and variability for sample size calculation, rather than for comparative analysis between treatment protocols. Mean bladder constraints, rectal constraints, and bladder volume (mL) were calculated. The association slopes between bladder constraints and bladder volume and between rectal constraints and bladder volume were calculated using a multilevel mixed-effects linear regression model with individual patients as random effects. The association slopes (± standard deviation) were −0.05 (0.01) for bladder and −0.01 (0.01) for rectum. At 90% statistical power, the calculated sample sizes compared with the null hypothesis of no association (slope = 0) were 4 for bladder and 11 for rectum.
Because the primary analysis was conducted at the session level using repeated measurements, the effective number of observations for the regression model was increased beyond the number of individual patients. To account for within-patient correlation, multilevel mixed-effects models with patient-level random effects were applied.
However, the pilot study was based on a small and imbalanced sample, particularly for the 60-Gy protocol, which may limit the precision of the estimated effect sizes. Therefore, while the calculated sample size was considered sufficient for detecting the primary association, subgroup analyses should be interpreted with caution due to potential limitations in statistical power.
| Results | ▴Top |
A total of 388 radiotherapy sessions were analyzed—308 across 11 patients treated with the 70 Gy protocol and 80 across four patients treated with the 60 Gy protocol—among 15 patients with localized prostate cancer who underwent CT simulation and completed treatment, with a corresponding CBCT image acquired at each session. The participant flow was presented in Figure 1. A summary of patient characteristics is shown in Table 1. No missing data were identified, as all information was recorded in either the electronic archiving system or the radiation planning system, and most variables were objective in nature.
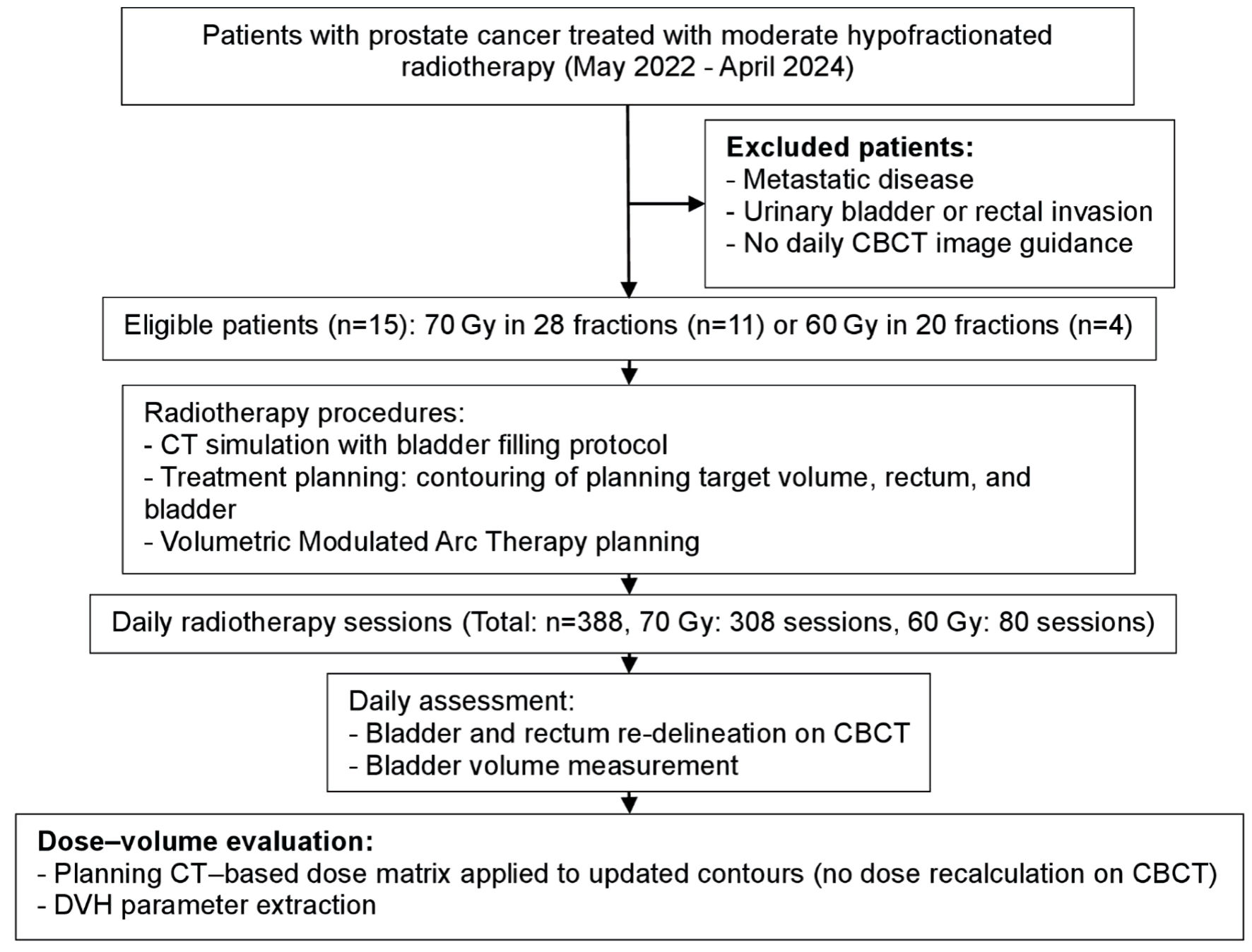 Click for large image | Figure 1. Participant flow diagram. CBCT: cone beam computed tomography; CT: computed tomography; DVH: dose–volume histogram. |
 Click to view | Table 1. Patient Characteristic |
The variation in bladder volume for each patient showed that the range of planning volumes for the 70-Gy and 60-Gy protocols were 45.3–298.6 mL (mean ± standard deviation (SD): 153.8 ± 81.4) and 63.4–382.4 mL (186.8 ± 145.1), respectively. The corresponding bladder volumes during the treatments ranged from 43.4 to 631.3 mL (195.6 ± 106.9) for the 70-Gy protocol, and 82–535.6 mL (209.56 ± 94.7) for the 60-Gy protocol. The average treatment bladder volume increased from 153.8 ± 81.4 mL (planning volume) to 195.6 ± 106.9 mL for the 70-Gy protocol (n = 11), and from 186.8 ± 145.1 mL (planning volume) to 209.56 ± 94.7 mL for the 60-Gy protocol (n = 4).
To graphically assess the association between bladder and OAR dose constraint, scatterplots, linear (fractional-polynomial) prediction plots, and locally weighted regression (LOWESS) plots between bladder volume and each bladder or rectal constraint were created and illustrated in Figures 2, 3 for 70-Gy protocol, and Figures 4, 5 for 60-Gy protocol. Vertical line at 200 mL bladder volume was illustrated as 200 mL bladder volume usually dictated as adequate pre-treatment bladder volume [15]. The correlation results were also presented in Table 2. Regarding the 70-Gy protocol, no above-threshold overdoses were detected for V79 and V74 of bladder constraints, and V74 of rectal constraints. However, significant correlation between bladder volume and percentage point of OAR constraints were detected in all the rest constraints level on both bladder and rectum in respect of the more bladder volume increased, percentage points of constraints decreased. Notably, the magnitude of this correlation was greater for bladder constraints, with risk differences ranging from −6.4% to −7.8% per 100 mL increase in bladder volume, compared to rectal constraints, which showed smaller risk differences of −1.0% to −2.2% per 100 mL. According to 60-Gy protocol, the significant correlation (bladder volume increased, constraints decreased) was detected only regarding urinary bladder. However, significant correlation was not detected regarding all rectal constraint levels. Table 2 presents bladder volume as a function of patients not being overdosed. At the 95 percentiles (i.e., 95% of treatment sessions were not overdosed), a bladder volume around 200 mL was usually adequate to protect overdosing, except for rectum (70-Gy protocol: 288.4 mL required for rectal V50; 60-Gy: 223 mL required for bladder V60, 228.9 mL for rectal V48.6, and 293.9 mL for rectal V60). To avoid overdose in 100% of sessions, the required bladder volume typically ranged from 200 to 300 mL, but could be as low as 125 mL or as high as 537.5 mL.
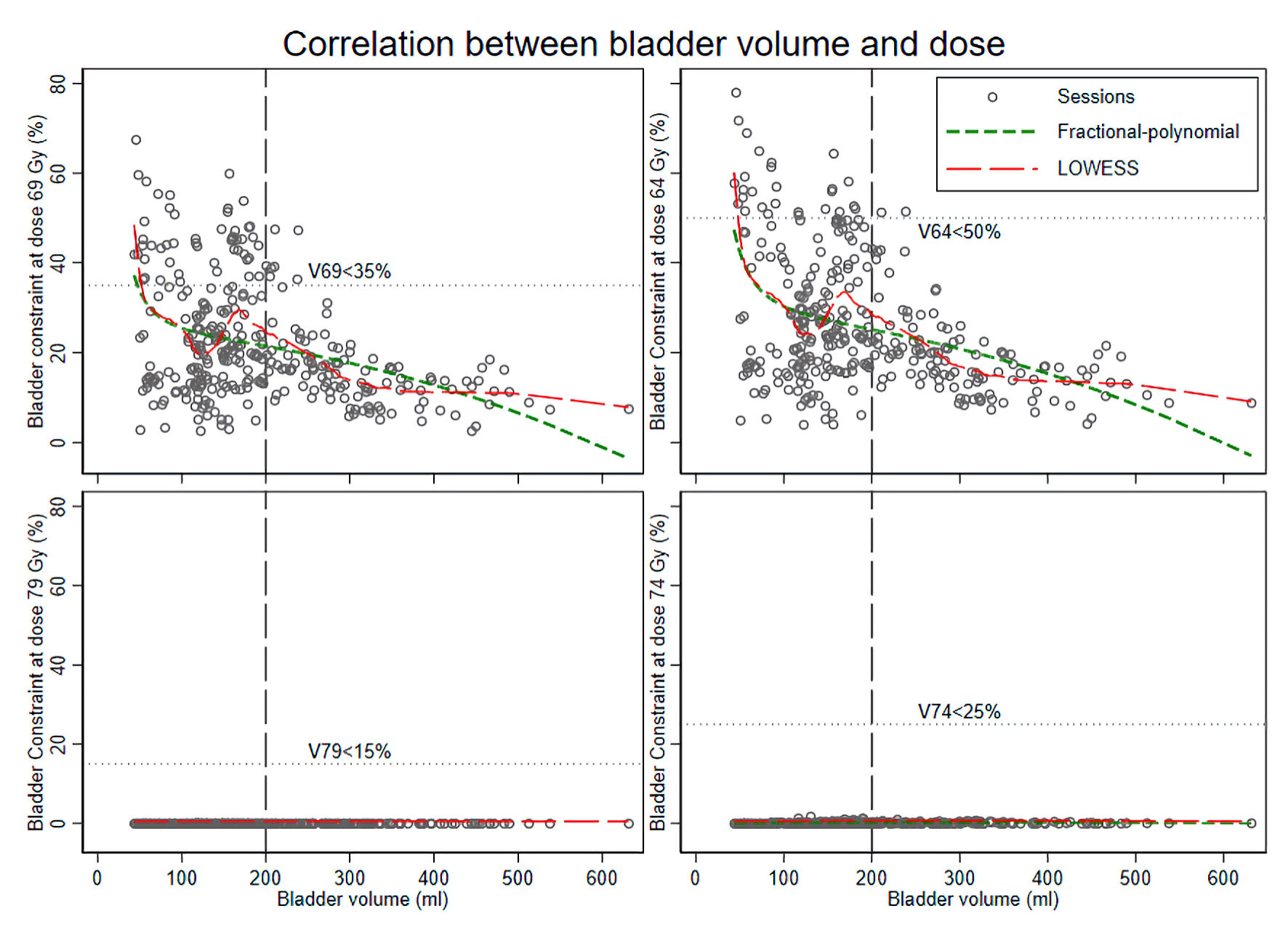 Click for large image | Figure 2. Correlation between bladder volume (mL) and bladder dose (dose–volume constraints) in the 70 Gy/28 fractions radiotherapy protocol. LOWESS: locally weighted regression plots. |
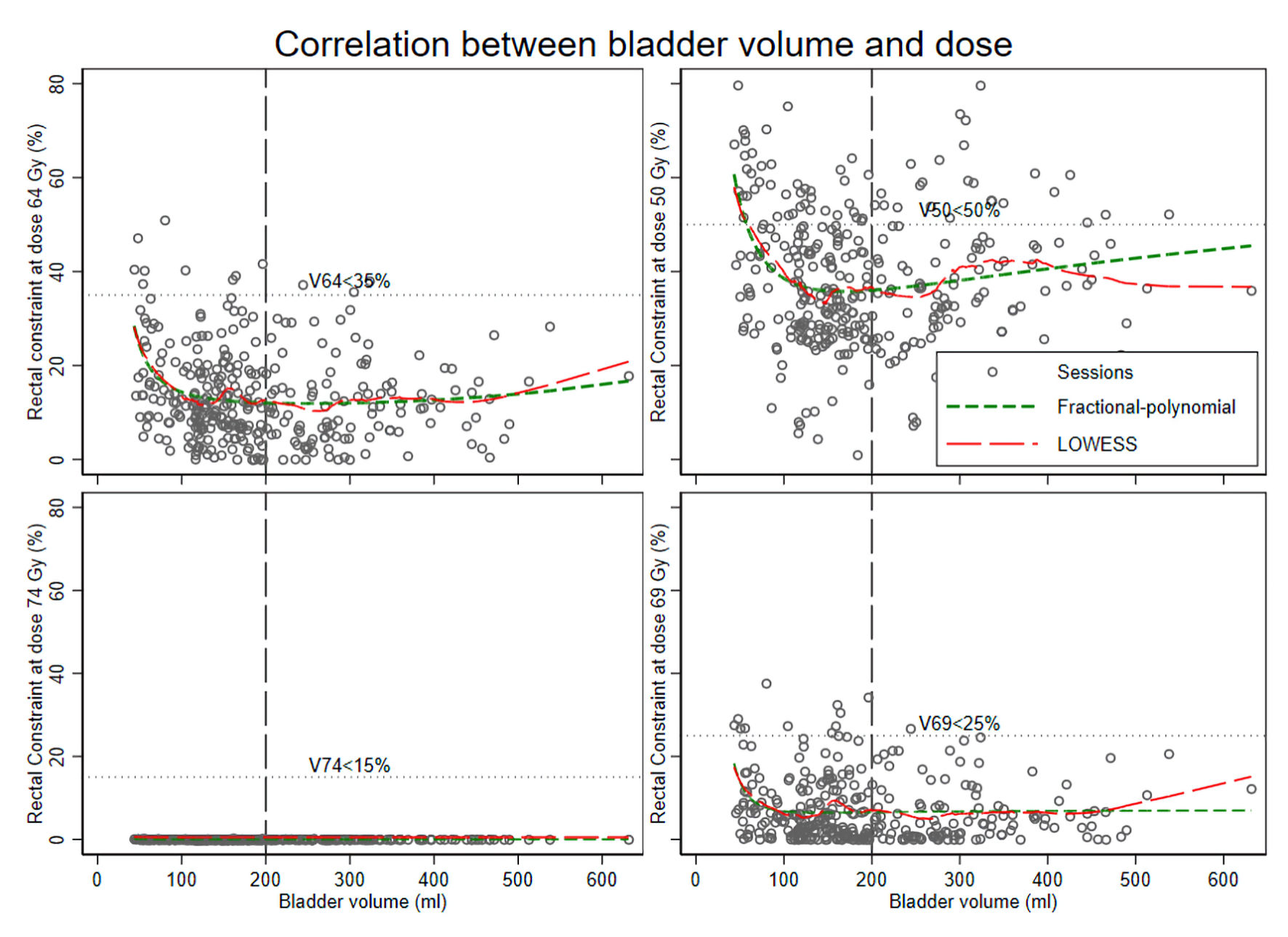 Click for large image | Figure 3. Correlation between bladder volume (mL) and rectal dose (dose–volume constraints) in the 70 Gy/28 fractions radiotherapy protocol. LOWESS: locally weighted regression plots. |
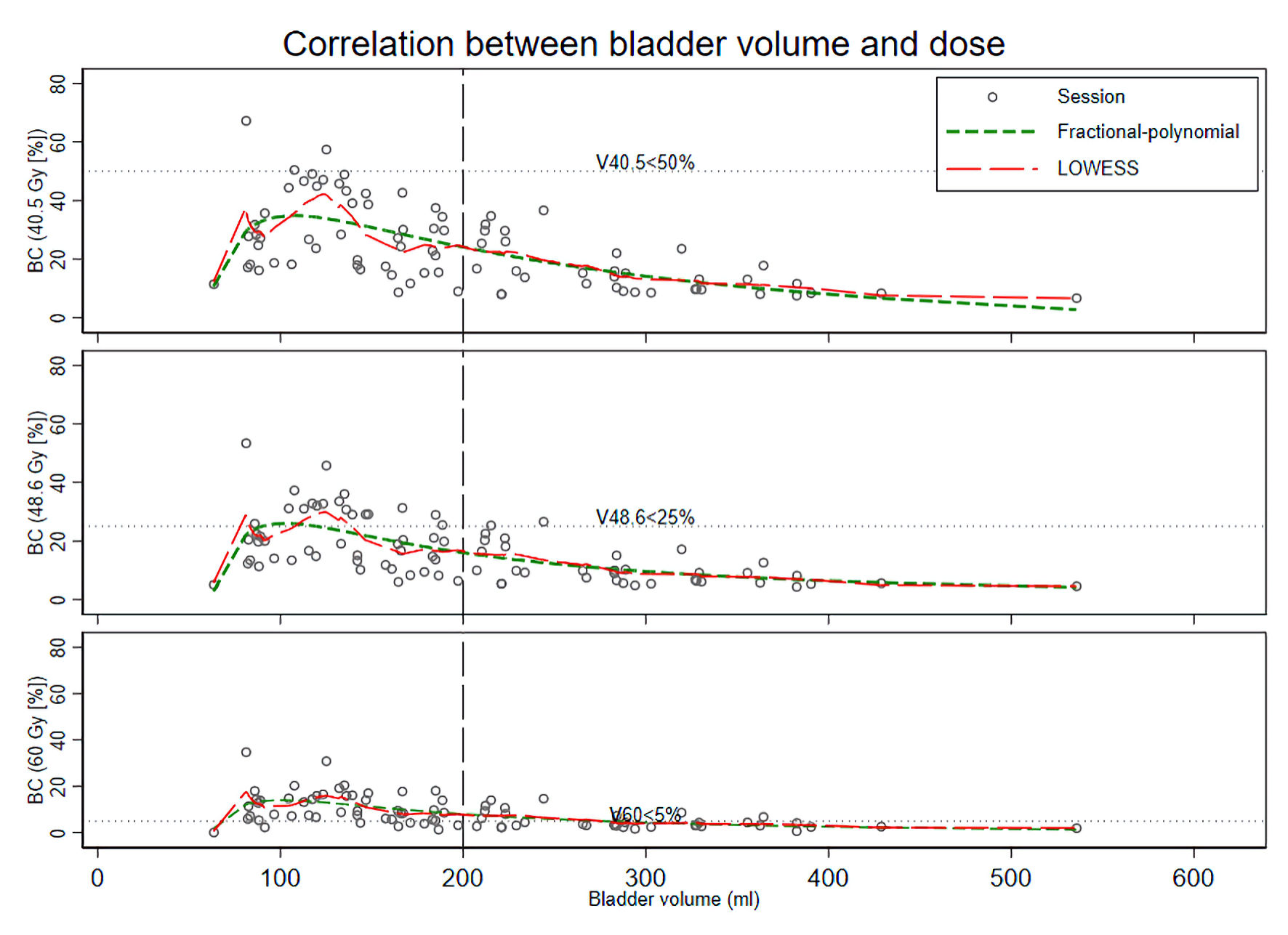 Click for large image | Figure 4. Correlation between bladder volume (mL) and bladder dose (dose–volume constraints) in the 60 Gy/20 fractions radiotherapy protocol. BC: bladder constraint; LOWESS: locally weighted regression plots. |
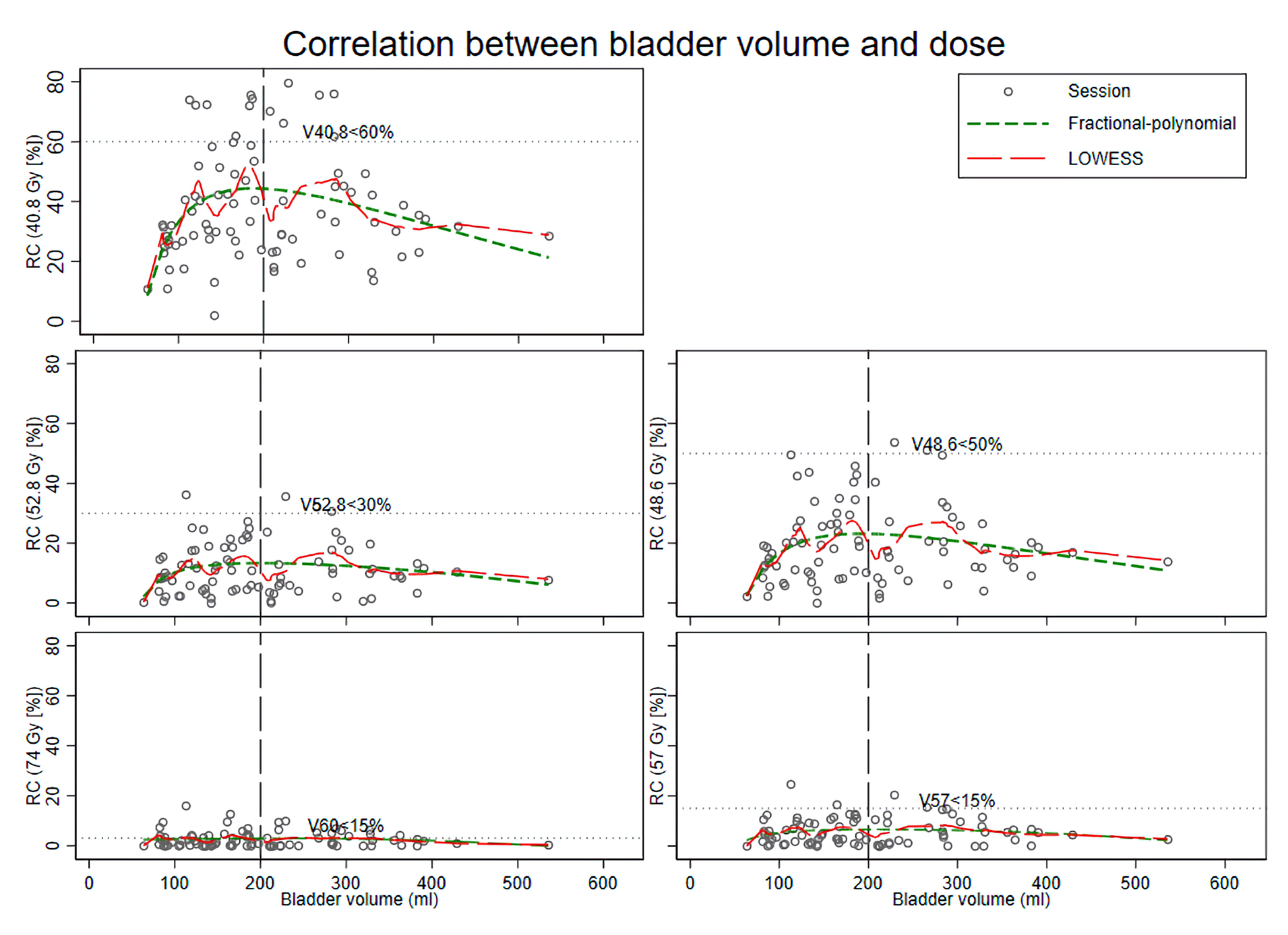 Click for large image | Figure 5. Correlation between bladder volume (mL) and rectal dose (dose–volume constraints) in the 60 Gy/20 fractions radiotherapy protocol. LOWESS: locally weighted regression plots; RC: rectal constraint. |
Click to view | Table 2. Bladder Volume Thresholds (95th and 100th Percentiles) and Adjusted Dose Constraint Correlations by Radiotherapy Protocol and Organ at Risk |
Our secondary objective was exploring factors related to exceeding OAR dose constraints in moderate hypofractionated radiotherapy (Table 3). Bladder volume was a significant protective over-dosed factor (risk ratio (RR) (95% confidence interval (CI)): 0.37 (0.17, 0.79)), while unfavorable/high prostate cancer recurrence risk and 60-Gy protocol were over-dosed risk (RR (95% CI): 2.41 (1.12, 5.16), 15.4 (2.93, 81.02), respectively) for urinary bladder as OAR. For the rectum, only 60-Gy protocol was a significant risk factor (RR (95% CI): 4.71 (1.45, 15.35)), while bladder volume was no longer a protective factor, although some protective trend was shown (RR (95% CI): 0.80 (0.50, 1.25)).
Click to view | Table 3. Association Between Patient and Treatment Factors and the Risk of Weighted Overdose Counts, Analyzed Using Zero-Inflated Poisson Regression |
Among the 15 participants, all experienced acute GI toxicity, with 13 patients presenting only grade I toxicity. Two of the four patients (50%) who received the 60-Gy protocol developed grade II rectal toxicity, which included rectal pain and diarrhea. Additionally, three patients in the 60-Gy group reported rectal discomfort during treatment, although none required medication. No chronic complications or urinary bladder toxicities were observed in this study.
| Discussion | ▴Top |
Our results demonstrated an inverse correlation between bladder volume and the percentage of radiation spillage to adjacent OARs, specifically the bladder and rectum. This suggests a protective effect, as larger bladder volumes were associated with lower radiation exposure to OARs—a concept supported by previous studies [4, 5, 16]. Recent studies have further evaluated the impact of anatomical variation and intrafraction motion on dosimetry during prostate radiotherapy [6, 7]. However, upon closer analysis, the protective effect of bladder filling was more pronounced for the urinary bladder in both the 70-Gy and 60-Gy protocols, with risk differences ranging from −3.1% to −7.8% per 100 mL increase in bladder volume. In contrast, the rectum exhibited only a modest protective effect under the 70-Gy protocol (risk differences around −1.0% to −2.2% per 100 mL), and no significant protective effect under the 60-Gy protocol. This may be explained by the fact that rectal dose is influenced by multiple anatomical factors, including rectal filling, gas distribution, and shape, which were not explicitly assessed in this study and may confound the relationship between bladder volume and rectal dose [17].
When evaluating the dose-volume histogram–defined overdose percentage across radiotherapy sessions by patient percentiles, the bladder volumes required to prevent overdosing in 95% and 100% of patients were generally consistent with these findings. In the 70-Gy protocol, the bladder volume needed to fully avoid rectal overdose (100th percentile) ranged from 243.9 to 537.5 mL, compared to a maximum of 238.2 mL needed for the urinary bladder. For the urinary bladder, achieving complete protection (100th percentile) in the 60-Gy protocol required larger bladder volumes (125–364.2 mL) than in the 70-Gy protocol.
These results highlight that bladder distention more effectively reduces dose to the urinary bladder than to the rectum, possibly due to anatomical displacement or dose conformality differences. These findings are consistent with prior studies reporting a higher incidence of rectal injury in prostate cancer radiotherapy, particularly with hypofractionated regimens [1]. Unlike studies that rely on comparisons between discrete bladder-filling states or on recalculated dose distributions using daily imaging [4, 7], our approach evaluates dose–volume constraint behavior across a continuum of bladder volumes using the original planning dose applied to daily anatomical variations. This framework may better reflect routine clinical workflows and provide complementary insight into the relationship between bladder volume and OAR dose constraints.
To contextualize our finding of a limited association between bladder filling volume and rectal dose, we identified few prior studies with mixed results. Moiseenko et al reported a small, non-significant reduction in rectal dose with a full bladder [10]. In contrast, Frizzell et al found a statistically significant reduction in mean rectal dose with a full versus empty bladder (25.41 Gy vs. 27.6 Gy; P = 0.031) [7]. Notably, Frizzell’s analysis compared two discrete bladder-filling states at planning [7], whereas our study evaluated the association across a continuum of bladder volumes over repeated fractions. Given these design differences and the small number of available comparative studies, larger prospective datasets are needed to determine whether bladder filling reliably reduces rectal dose across modern treatment regimens.
Study’s secondary outcome analyzes factors associated with OAR overdose in moderate hypofractionated radiotherapy. In general, patient factors associated with increased OAR overdose were older patient age, thinner body habitus, smoking, and certain medical comorbidities [18]. Radiation dose, fractionation, and field size were treatment-related factors [18]. We found that the 60-Gy protocol (a more hypofractionated schedule) and unfavorable or high prostate cancer recurrence risk were associated with increased risk of OAR overdose.
Among the patients who experienced clinical toxicity, grade II acute complications were observed in two of the four patients who received the 60-Gy protocol and were limited to rectal toxicity. While this observation is based on a small number of events and should be interpreted cautiously, it aligns with findings from a recent study by Tao et al [19], which included 187 participants and demonstrated that the 60-Gy protocol was associated with significantly higher rates of late grade 2 urinary toxicity and a non-significant trend toward increased acute GI toxicity. The survival benefit of 60 Gy was marginally non-significant [19]. However, the 60-Gy protocol has also been considered a standard schedule for patients with localized prostate cancer, as demonstrated in multiple clinical trials with acceptably low toxicity profiles [20]. In light of this existing evidence, our findings suggest that while the 60-Gy protocol may be associated with higher rates of OAR overdose based on dose-volume metrics, this may not directly reflect clinical toxicity rates. Notably, a formal analysis linking toxicity outcomes with dose–volume constraint violations was not performed due to the limited number of patients and observed events. Therefore, the toxicity findings should be interpreted descriptively, and further studies with larger sample sizes are needed to better evaluate the relationship between dosimetric parameters and clinical outcomes.
Our secondary findings were also consistent with the primary results, indicating that bladder volume served as a protective factor against radiation spillage. However, these associations were statistically significant only for the urinary bladder as an OAR, and not for the rectum. These findings further emphasize the importance of achieving adequate bladder filling prior to radiotherapy, carefully selecting the radiation protocol, and ensuring precise organ delineation during CT-based treatment planning, as well as evaluating rectal protection strategies such as spacers or rectal balloons—particularly when considering ultra-hypofractionated protocols [21].
Interestingly, urinary bladder filling time was not a significant predictive factor. This may be due to the close correlation between bladder volume and filling time, as well as the relatively uniform filling durations across patients resulting from adherence to the standardized 40–60 min protocol. However, the findings may also suggest that bladder filling time alone is an unreliable indicator of actual bladder volume. Based on these results, using ultrasound to assess bladder volume before each radiotherapy session may provide a more accurate and consistent measure than relying on filling time alone [22].
A key strength of our study is that it reflects real-world clinical practice and accounts for repeated radiotherapy sessions in individual patients when evaluating the correlation between bladder volume and OAR dose constraints.
However, our study also had several important limitations. The most significant was its method-oriented design, in which the primary outcomes focused on dose–volume constraints for OARs derived from dose–volume histogram (DVH) data, rather than direct clinical outcomes. Although we attempted to provide clinical context by reporting 1-year radiation-induced morbidity, the applicability to real-world clinical practice remains limited. Our aim was to illustrate, in detail, how radiation may spill over to OARs under varying bladder volumes, while incorporating elements of clinical relevance. In light of this limitation, applying findings from published studies or conducting future research with a stronger focus on clinical outcomes may enhance practical applicability.
Second, while DVH metrics were used to quantify dose constraints to OARs, they do not account for spatial distribution of the dose within the organ. Thus, regions receiving high doses near critical substructures (e.g., anterior rectal wall) may not have been adequately captured [23].
Another important limitation relates to the dose evaluation method and potential confounding from baseline treatment planning. In this study, the original planning CT–based dose distribution was applied to organ contours derived from daily CBCT images, without dose recalculation. Therefore, the estimated dose–volume parameters may not fully represent the actual delivered dose under daily anatomical variations, as this approach does not account for tissue heterogeneity, anatomical deformation, or changes in beam attenuation. In addition, baseline treatment plan quality and proximity to dose–volume constraint thresholds were not explicitly accounted for. Patients whose initial plans were closer to constraint limits may have been more likely to exceed these thresholds during daily anatomical variation. Variability in treatment planning practices may also influence dose distribution and organ-at-risk exposure. Variations in PTV, including differences in target size and inclusion of seminal vesicles in higher-risk patients, were also not explicitly accounted for and may act as additional confounding factors. However, this framework allows for the assessment of how anatomical variation alone influences dose–volume constraint behavior under a fixed treatment plan, which may reflect practical clinical workflows where routine CBCT-based dose recalculation is not performed.
Third, the sample size was calculated based on our primary objective—evaluating the correlation between bladder volume and OAR constraints. As a result, the secondary outcomes assessing factors affecting OAR overdose should be interpreted as supportive findings, as the study may not have been adequately powered to detect significant associations. Although the analysis included repeated measurements across treatment sessions, the number of individual patients—particularly in the 60-Gy group (n = 4)—was limited. As a result, subgroup comparisons may be underpowered, and the observed differences between protocols may reflect statistical instability rather than true clinical differences. Moreover, the number of participants receiving the 60-Gy protocol did not reach the calculated minimum sample size of 11 patients required for rectal analysis, although it was adequate for bladder analysis (minimum required: four patients). Therefore, analyses within this subgroup may have limited statistical power, and the slightly different results observed with the 60-Gy protocol should be interpreted with caution, as they may partly reflect the smaller sample size rather than true differences between protocols. However, the dataset still included approximately 80 treatment fractions from patients treated with the 60-Gy protocol, which may provide preliminary insight into the potential relationship between bladder volume and OAR dose–volume constraints.
Fourth, as a retrospective observational cohort study, our design is inherently susceptible to certain biases—such as selection bias, protocol assignment bias, and measurement bias. In addition, important patient-related factors such as smoking status, alcohol consumption, body mass index, and comorbidities were not available in the dataset. These factors may influence organ motion, anatomy, and radiation tolerance, and their absence may limit the ability to fully adjust for potential confounding. However, most of the primary variables in this study (e.g., bladder volume and DVH parameters) were objectively measured from imaging and treatment planning systems. Therefore, while these limitations may introduce residual confounding, the findings are considered to reasonably reflect real-world clinical practice, particularly in the context of protocol selection.
Finally, this study focused primarily on the urinary bladder and rectum, as these organs are located adjacent to the prostate and are among the OARs most commonly exposed to clinically significant radiation doses during prostate radiotherapy. Other structures that may also be affected by radiation exposure, such as the penile bulb and femoral heads, were not evaluated [24]. In addition, the present analysis did not assess the impact of bladder volume variation on target coverage or prostate dose. Changes in bladder filling may influence prostate position and internal anatomy, potentially affecting the delivered dose distribution to the target volume [25]. Therefore, the findings of this study should be interpreted primarily in the context of organ-at-risk dose constraints. The potential impact of bladder volume variation on target coverage and prostate dosimetry was not evaluated and warrants consideration when interpreting the overall dosimetric consequences of bladder filling during prostate radiotherapy.
Conclusions
Increased bladder volume was associated with a protective effect, reducing radiation dose exposure to adjacent OARs, including the bladder and rectum. However, this protective association was less pronounced for the rectum—particularly under the 60-Gy protocol. Further clinical studies are warranted to validate these findings, and integration with insights from existing published research may help guide their application in routine clinical practice.
Acknowledgments
None to declare.
Financial Disclosure
The authors received financial support from Sawanpracharak Hospital Medical Education Center.
Conflict of Interest
All authors declare that there is no conflict of interest.
Informed Consent
The requirement for informed consent was waived by the Sawanpracharak Hospital Ethical Committee due to the retrospective observational study design.
Author Contributions
All authors made substantial contributions to this manuscript. All authors conceived and designed the study. NS, ST and JP were responsible for the statistical analysis. All authors participated in drafting the manuscript, critically revising it, and approving the final version.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
| References | ▴Top |
- Morgan SC, Hoffman K, Loblaw DA, Buyyounouski MK, Patton C, Barocas D, Bentzen S, et al. Hypofractionated radiation therapy for localized prostate cancer: an ASTRO, ASCO, and AUA evidence-based guideline. J Clin Oncol. 2018;36(34):JCO1801097.
doi pubmed - Benjamin LC, Tree AC, Dearnaley DP. The Role of Hypofractionated Radiotherapy in Prostate Cancer. Curr Oncol Rep. 2017;19(4):30.
doi pubmed - Chanayota J, Suriyapee S, Alisanant P, Sanghangthum T. Dosimetric comparison between using daily cone beam CT and planning CT in volumetric modulated arc therapy technique for prostate cancer therapy. J Phys Conf Ser. 2019;1248(1):012044.
- Pearson D, Gill SK, Campbell N, Reddy K. Dosimetric and volumetric changes in the rectum and bladder in patients receiving CBCT-guided prostate IMRT: analysis based on daily CBCT dose calculation. J Appl Clin Med Phys. 2016;17(6):107-117.
doi pubmed - Casares-Magaz O, Moiseenko V, Hopper A, Pettersson NJ, Thor M, Knopp R, Deasy JO, et al. Associations between volume changes and spatial dose metrics for the urinary bladder during local versus pelvic irradiation for prostate cancer. Acta Oncol. 2017;56(6):884-890.
doi pubmed - Roch M, Zapatero A, Castro P, Hernandez D, Chevalier M, Garcia-Vicente F. Dosimetric impact of rectum and bladder anatomy and intrafractional prostate motion on hypofractionated prostate radiation therapy. Clin Transl Oncol. 2021;23(11):2293-2301.
doi pubmed - di Franco F, Baudier T, Pialat PM, Munoz A, Martinon M, Pommier P, Sarrut D, et al. Ultra-hypofractionated prostate cancer radiotherapy: Dosimetric impact of real-time intrafraction prostate motion and daily anatomical changes. Phys Med. 2024;118:103207.
doi pubmed - Schober P, Vetter TR. Repeated measures designs and analysis of longitudinal data: if at first you do not succeed-try, try again. Anesth Analg. 2018;127(2):569-575.
doi pubmed - Frizzell B, Lovato J, Foster J, Towers A, Lucas J, Able C. Impact of bladder volume on radiation dose to the rectum in the definitive treatment of prostate cancer. J Community Support Oncol. 2015;13(8):288-291.
doi pubmed - Moiseenko V, Liu M, Kristensen S, Gelowitz G, Berthelet E. Effect of bladder filling on doses to prostate and organs at risk: a treatment planning study. J Appl Clin Med Phys. 2006;8(1):55-68.
doi pubmed - Lee WR, Dignam JJ, Amin M, Bruner D, Low D, Swanson GP, Shah A, et al. NRG Oncology RTOG 0415: a randomized phase III non-inferiority study comparing two fractionation schedules in patients with low-risk prostate cancer. J Clin Oncol. 2016;34(2_suppl):1-1.
- Dearnaley D, Syndikus I, Sumo G, Bidmead M, Bloomfield D, Clark C, Gao A, et al. Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: preliminary safety results from the CHHiP randomised controlled trial. Lancet Oncol. 2012;13(1):43-54.
doi pubmed - Eade TN, Horwitz EM, Ruth K, Buyyounouski MK, D'Ambrosio DJ, Feigenberg SJ, Chen DY, et al. A comparison of acute and chronic toxicity for men with low-risk prostate cancer treated with intensity-modulated radiation therapy or (125)I permanent implant. Int J Radiat Oncol Biol Phys. 2008;71(2):338-345.
doi pubmed - Lee AH, Wang K, Scott JA, Yau KK, McLachlan GJ. Multi-level zero-inflated poisson regression modelling of correlated count data with excess zeros. Stat Methods Med Res. 2006;15(1):47-61.
doi pubmed - Pang EPP, Knight K, Hussain A, Fan Q, Baird M, Tan SXF, Mui WH, et al. Reduction of intra-fraction prostate motion - Determining optimal bladder volume and filling for prostate radiotherapy using daily 4D TPUS and CBCT. Tech Innov Patient Support Radiat Oncol. 2018;5:9-15.
doi pubmed - Chen Z, Yang Z, Wang J, Hu W. Dosimetric impact of different bladder and rectum filling during prostate cancer radiotherapy. Radiat Oncol. 2016;11:103.
doi pubmed - van der Walle R, Staal FHE, Janssen J, Langendijk JA, Brouwer CL, Aluwini S. Toxicity of rectal preparation strategies in ultra-hypofractionated SBRT for prostate cancer. Tech Innov Patient Support Radiat Oncol. 2026;38:100405.
doi pubmed - Shadad AK, Sullivan FJ, Martin JD, Egan LJ. Gastrointestinal radiation injury: symptoms, risk factors and mechanisms. World J Gastroenterol. 2013;19(2):185-198.
doi pubmed - Tao Y, Cheng W, Zhen H, Shen J, Guan H, Hou X, Hu K, et al. Moderate-hypofractionated radical radiotherapy for early-stage prostate cancer: a propensity score matching analysis comparing dose fractionation patterns. Cancer Control. 2025;32:10732748251330058.
doi pubmed - Dearnaley D. Moderate hypofractionated radiotherapy for localised prostate cancer: a new standard of care. Cancer Radiother. 2025;29(5-6):104678.
doi pubmed - Serrano NA, Kalman NS, Anscher MS. Reducing rectal injury in men receiving prostate cancer radiation therapy: current perspectives. Cancer Manag Res. 2017;9:339-350.
doi pubmed - Smith L, Gittins J, Ramnarine KV, Chung E. Assessment of an ultrasound bladder scanner in prostate radiotherapy: A validation study and analysis of bladder filling variability. Ultrasound. 2022;30(1):36-43.
doi pubmed - Casares-Magaz O, Moiseenko V, Witte M, Rancati T, Muren LP. Towards spatial representations of dose distributions to predict risk of normal tissue morbidity after radiotherapy. Phys Imaging Radiat Oncol. 2020;15:105-107.
doi pubmed - Le Guevelou J, Zilli T. Prostate cancer radiotherapy and incidental testicular irradiation: Impact on gonadal function. Clin Transl Radiat Oncol. 2023;40:100611.
doi pubmed - Chauhan K, Ebner DK, Tzou K, Ryan K, May J, Kaleem T, Miller D, et al. Assessment of bladder filling during prostate cancer radiation therapy with ultrasound and cone-beam CT. Front Oncol. 2023;13:1200270.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
World Journal of Nephrology and Urology is published by Elmer Press Inc.