| World Journal of Nephrology and Urology, ISSN 1927-1239 print, 1927-1247 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Nephrol Urol and Elmer Press Inc |
| Journal website https://wjnu.elmerpub.com |
Review
Volume 15, Number 3, July 2026, pages 55-64

Kidney Health for All: Caring for People, Protecting the Planet
Raymond Vanholdera, b, Dina Abdellatifc, Augusto Cesar Soares Dos Santos Jrd, e, Ricardo Correa-Rotterf, Natarajan Gopalakrishnang, Bill Wangh, Stefanos Roumeliotisi, n, Alessandro Balduccij, Agnes Harisk, Manjusha Yadlal, Li-Li Hsiaom
aNephrology Section, Department of Internal Medicine and Pediatrics, Ghent University Hospital, Ghent, Belgium
bEuropean Kidney Health Alliance, Brussels, Belgium
cDepartment of Nephrology, Cairo University Hospital, Cairo, Egypt
dFaculdade Ciencias Medicas de Minas Gerais, Belo Horizonte, Minas Gerais, Brazil
eHospital das Clinicas, Ebserh, Universidade Federal de Minas Gerais, Minas Gerais, Brazil
fInstituto Nacional de Ciencias Medicas y Nutricion Salvador Zubiran, Mexico City, Mexico
gTransplant Authority of Tamil Nadu, Chennai, India
hHong Kong Kidney Foundation, Hong Kong, SAR, China
i2nd Department of Nephrology, AHEPA University Hospital, Medical School, Aristotle University of Thessaloniki, Greece
jItalian Kidney Foundation Italy, Rome, Italy
kDepartment of Internal Medicine and Nephrology, Peterfy Hospital, Budapest, Hungary
lDepartment of Nephrology, Gandhi Medical College, Hyderabad, Telangana, India
mRenal Division, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA
nCorresponding Author: Stefanos Roumeliotis, 2nd Department of Nephrology, AHEPA Hospital, Medical School, Aristotle University of Thessaloniki, 54636 Thessaloniki, Greece
Manuscript submitted April 16, 2026, accepted April 24, 2026, published online July 8, 2026
Short title: Kidney Health for All
doi: https://doi.org/10.14740/wjnu1053
| Abstract | ▴Top |
The current kidney care model, focused on late-stage disease and in-center hemodialysis, is unsustainable, because of costs, environmental burden, poor outcomes, and reduced quality of life. The 78th World Health Assembly’s recognition of kidney disease as a serious health threat presents a critical opportunity to reshape kidney care. Aligned with this, the 2026 World Kidney Day theme, “Kidney Health for All: Caring for People, Protecting the Planet”, calls for a systematic change. A sustainable model must prioritize early detection and prevention, reducing the need for kidney replacement therapy. Transplantation and home dialysis benefit people with kidney failure, environment, and society. Dialysis itself must become more eco-friendly without compromising care quality, recognizing that planetary perturbations in turn affect kidney health. Conservative care should also be considered, particularly for elderly and frail patients, if the quality-of-life benefits outweigh the perspectives offered by dialysis. Achieving this shift requires coordinated action across all stakeholders; education and engagement of the public, policy makers, and health professionals to raise awareness about the threat of kidney disease; and an urgent move toward patient-centered care.
Keywords: Environment; Green nephrology; Prevention; Screening; Sustainable kidney care; World Kidney Day
| Introduction | ▴Top |
Chronic kidney disease (CKD) is one of the most common noncommunicable diseases globally [1, 2], linked to significant comorbidities, particularly cardiovascular disease, premature mortality, societal costs, reduced productivity, and a considerable environmental footprint [3]. CKD disproportionately affects disadvantaged populations and minority groups [4]. Advanced CKD causes distressing symptoms, social isolation, and, in children, growth and development delays.
Despite its wide-ranging impact, CKD remains underrecognized as a global health threat. Recently, CKD’s profile was raised by the World Health Organization Resolution on Kidney Health, approved at the 78th World Health Assembly [5]. The Resolution urges governments to integrate prevention, early detection, and management of kidney disease into national noncommunicable disease strategies, and to expand access to equitable, sustainable, high-quality kidney care, progressively including dialysis, transplantation, and conservative care within universal health coverage. In addition, World Kidney Day (WKD) was acknowledged as key for raising public awareness and promoting kidney health.
Sponsored and championed by Guatemala, the Resolution marked a pivotal step in establishing kidney disease as a global health priority. Guatemala’s leadership was pivotal in mobilizing broad support, particularly from those countries most affected by the growing burden of CKD and care access inequities. It also recognized the strong influence of environmental factors on kidney health, highlighting the disproportionate impact of climate change on developing countries and small island States, as emphasized in the 77th WHA Resolution (see below).
These milestones form the policy foundation for the 2026 WKD theme, “Kidney Health for All: Caring for People, Protecting the Planet,” which underscores the need to safeguard kidney health, to address the environmental effect on kidney health but also of kidney care on the environment, and to pivot health care models from a focus on late-stage treatment to early risk reduction and detection (Fig. 1).
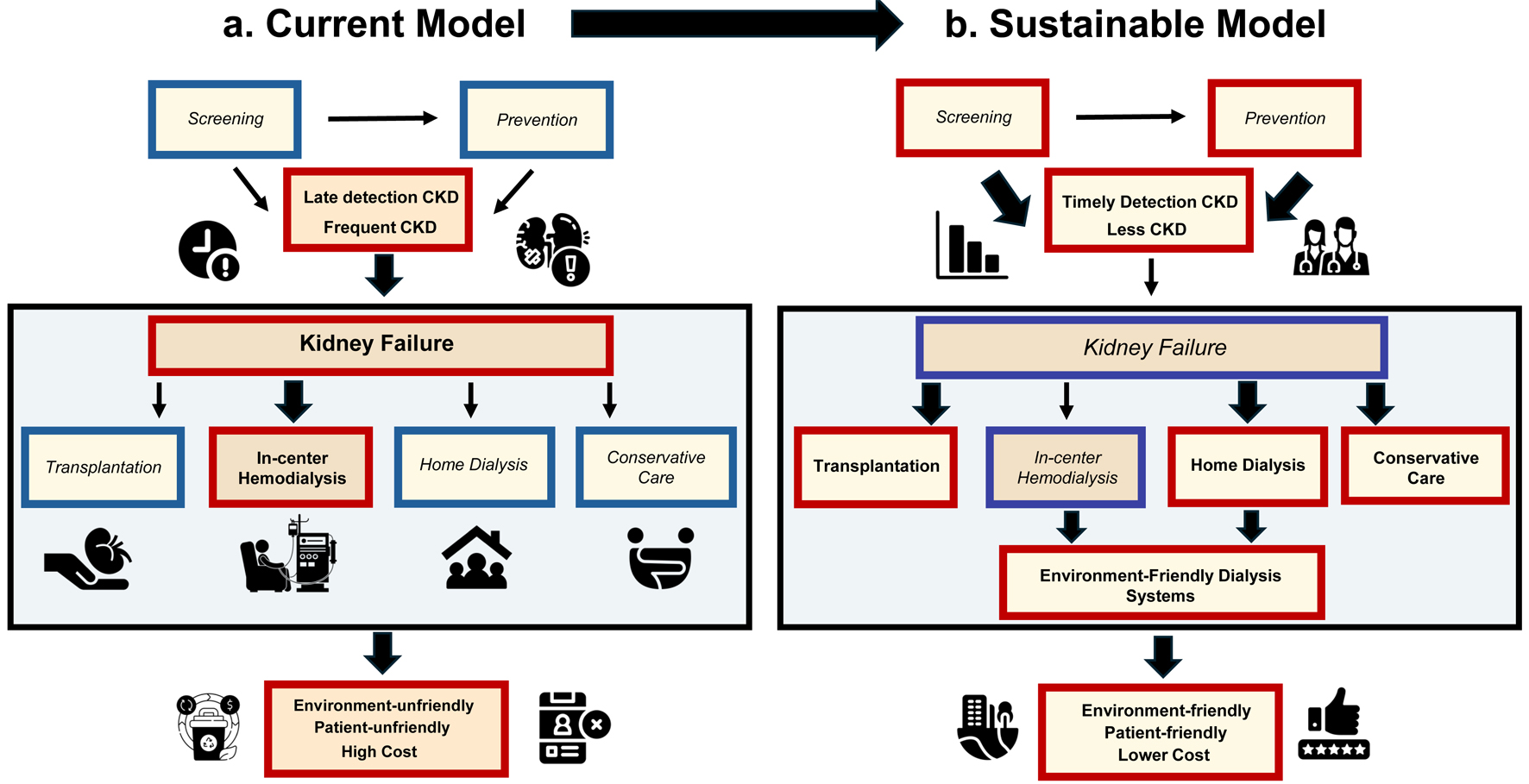 Click for large image | Figure 1. (a) Current model of kidney care. (b) Sustainable model of kidney care. Elements that are less or insufficiently prominent in that specific model are in italics with a blue frame; elements that are prominent in a specific model are in bold with a red frame. Yellow background indicates if beneficial for sustainability, and orange background indicates disadvantageous. Light blue–shaded box with black frame is used for kidney replacement therapy. The thickness of the arrows indicates the degree of impact on the following element. CKD: chronic kidney disease; home dialysis, peritoneal dialysis, and/or home hemodialysis. |
This editorial calls for urgent, integrated action across early detection, prevention, equitable care, and environmental stewardship to advance both kidney and planetary health (Table 1) [6], underscoring the need for a more sustainable kidney care model with prevention and ecofriendliness as two main pillars (Figs. 1 and 2) [6], to which all other attention points are linked. We offer a general outline of measures that can be taken by communities and governments, although it is merely impossible to propose a ready-made outline that fits all. Kidney health plans need to be developed, aiming for a sustainable model, but might necessitate adaptations depending on the local possibilities and circumstances.
 Click to view | Table 1. Different Actions to Make Kidney Care Sustainable, According to the Topic and Target |
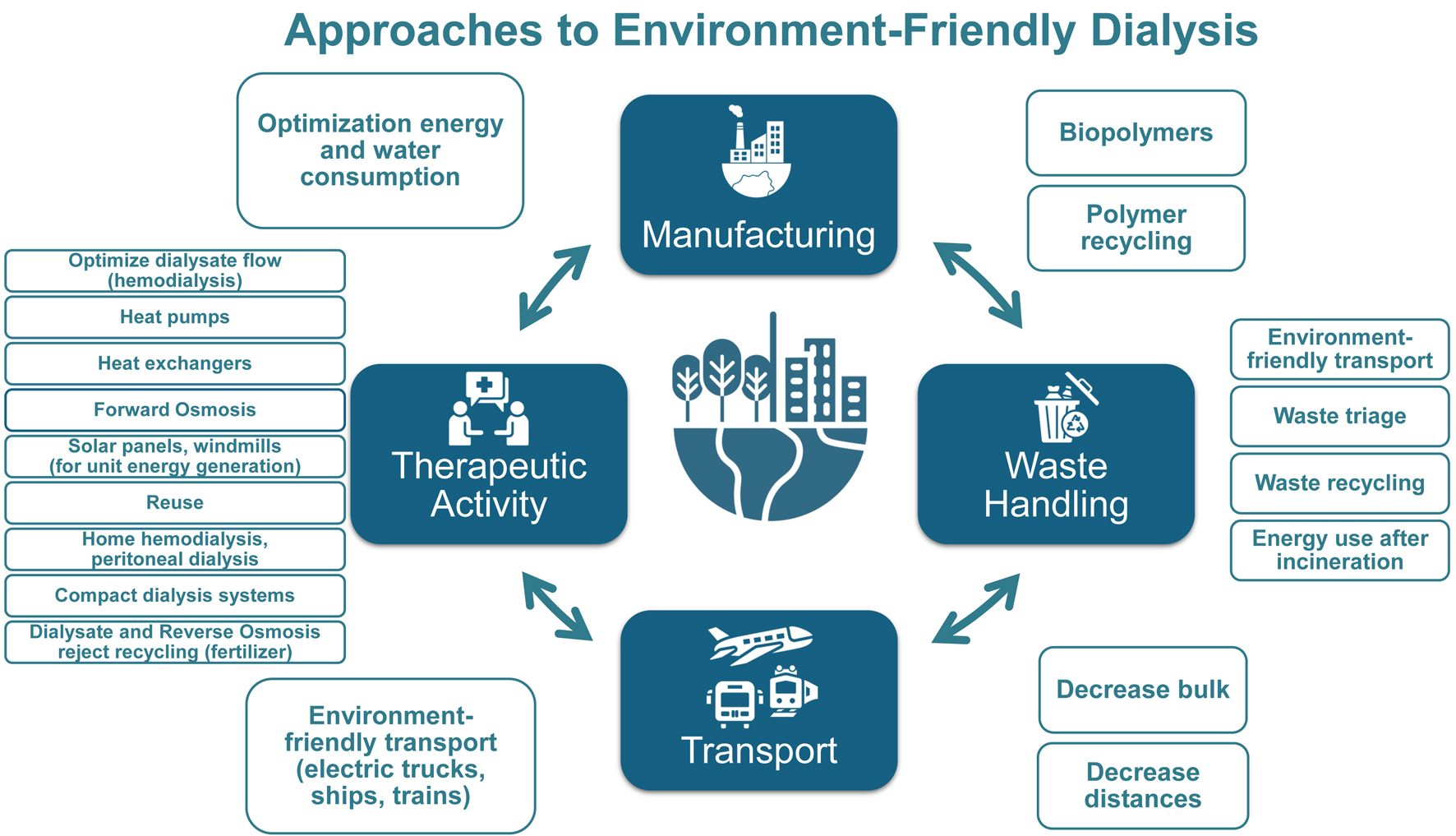 Click for large image | Figure 2. Approaches toward environment-friendly dialysis, categorized for manufacturing, transport, therapeutic activity, and waste handling. The list is not exhaustive. For more detailed lists, see the study by Vanholder et al [6]. Environment friendliness should not be pursued at the expense of patient quality of life or clinical status. Compact dialysis systems consume less water or recycle dialysate over sorbents. |
| Prevention: The Foundation of Kidney Health | ▴Top |
Beyond general primary and secondary preventive measures for all kidney conditions, prevention may require targeted therapies, including rare kidney diseases [7]. Diabetes and hypertension—the leading causes of CKD—remain widely underdiagnosed and undertreated [8]. Kidney function is further compromised by modifiable lifestyle factors, including smoking, unhealthy nutritional habits (notably, excess sugar and salt), alcohol use, obesity, exposure to nephrotoxins, physical inactivity, exposure to heat, environmental pollution, and agrochemicals. Addressing these could significantly reduce the CKD burden [9]. Prevention is beneficial across all country wealth levels but is especially critical where costly CKD therapies are inaccessible or inadequately reimbursed, resulting in premature death and catastrophic out-of-pocket health expenditures.
A shift toward prevention as the cornerstone to sustainable kidney care calls for simple, yet effective, public health strategies, such as promoting healthy diets or introducing health-oriented taxation (e.g., salt, sugar, or fat taxes) [9]. Currently, governments invest manifold more in cure than in prevention, and a more balanced distribution among both factors is needed. Several governments take steps in that direction, sometimes in the context of a global cardiovascular health plan, but approaches differ depending on the local conditions.
WKD promotes eight golden rules for kidney health—simple, actionable lifestyle measures [10]: regular physical activity; healthy diet; adequate hydration; blood glucose control; blood pressure management; avoiding smoking; using medications as prescribed; and regular kidney function testing. These principles provide a framework for kidney health promotion across populations and health care settings.
Because unfavorable living conditions and difficulties to reach quality care have a negative impact on outcomes of noncommunicable diseases, including CKD [11], prevention must also address social dimensions. These include food insecurity, poor food quality, poverty, remoteness (rural vs. urban), inadequate access to services, red lining, unfavorable living conditions (unhygienic and unsafe housing, inadequate building cooling, and polluted living areas), and lack of neighborhood greenery.
Public understanding of how the kidney functions and its threats is poor. Informative campaigns, like the European Renal Association’s ABCDE initiative, highlighting albuminuria, blood pressure, cholesterol, diabetes, and estimated glomerular filtration rate as key warning signs, should be widely disseminated [12]. The public is to be encouraged to ask their primary care providers about these factors, like people currently do for their glucose and cholesterol.
However, educational outreach often misses those at highest risk of CKD: individuals with limited health literacy, language or cultural barriers, or lower socioeconomic status. Tailored approaches (videos, social media campaigns, and cartoons) are vital to reach these deprived populations regarding all aspects and levels of CKD.
| Early Detection: A Critical, Underutilized Tool | ▴Top |
CKD symptoms typically emerge at advanced stages, when therapies often only can delay, not prevent, kidney failure [13, 14]. Serum creatinine remains the most widespread marker for routine assessment and monitoring of CKD but lacks sensitivity for early detection [15], although this is essential to timely and effectively prevent progression. Albuminuria stands out as a simple, low-cost, and reliable early indicator of kidney microvascular damage and CKD, but also of related conditions, such as hypertension, diabetes, and dyslipidemia [16]. However, urinary screening assessments, including albuminuria checks, are rarely performed, even in well-developed health care systems [17].
Albuminuria testing can thus detect hidden cases across the entire cardio-kidney-metabolic spectrum [16], serving as an alarm for conditions that, if untreated, lead to irreparable organ damage, including the kidneys. The progression of all conditions thus detected can be decelerated therapeutically, with the potential to reduce the pressing individual and societal burden of CKD and kidney failure. Modeling suggests that population-wide timely albuminuria screening and treatment could lower the lifetime incidence of dialysis or transplantation by 21.8% and of cardiovascular disease by 12% [18, 19]. Implementing universal screening from age 45 years or even 35 years onward has been suggested to enhance cost-effectiveness and health care resilience [18]. Programs like the US Kidney Disease Screening and Awareness Program help to promote early screening and detection of CKD [20].
In addition, kidney disease should be a central attention point also outside nephrology, particularly in diabetes, hypertension, cardiovascular disease, and obesity, as a negative outcome accelerator in these conditions [21, 22]. Underlining this threat needs continued advocacy of the nephrological community [23], particularly as there are now several novel therapies to delay progression [24]. For screening to have impact, it must be paired with education of the public and of frontline providers, such as general practitioners, nurses, pharmacists, and, particularly in low-resource settings, community health workers. Detection of CKD and its risk factors should be followed by effective therapies, given their wide-ranging benefits, but these should be made universally accessible and affordable.
Despite its growing burden, awareness and early detection of CKD remain limited in low- and middle-income countries. A 2024 pilot study in high-risk groups in India reported 60% prevalence but extremely low awareness (16.5% in rural areas; 1.4% in urban areas) [25]. In Brazil, serum creatinine and albuminuria testing remains below recommended levels, limiting early CKD detection and opportunities for timely intervention [26]. These gaps underscore the urgent need to integrate essential screening tests, like albuminuria and serum creatinine, into routine primary care, especially in regions where people often present with advanced disease.
| Environmental Risks: An Emerging Challenge for Kidney Health | ▴Top |
We are witnessing rapid environmental and climatologic changes with profound health consequences. The kidneys—which are central to maintaining volume homeostasis—are especially vulnerable for these shifts.
Global warming raises the risk of heat stress and dehydration, which are major contributors to acute kidney injury and kidney stone development [27, 28], and eventually progression to CKD [29]. Outdoor workers exposed to extreme heat are particularly at risk, especially when hydration is inadequate or working conditions are insufficiently adapted, as in Mesoamerican nephropathy, a rapidly progressing form of CKD identified in agricultural workers in (sub)tropical climates [30].
Climate change also intensifies extreme weather events, such as floods, hurricanes, and typhoons. These, combined with the rising temperatures, increase the spread of tropical diseases, like malaria or dengue, as well as water-borne disorders, like leptospirosis or infectious diarrhea [31], all of which can cause acute kidney injury. Flood waters may also become nephrotoxic when contaminated with industrial or natural pollutants. Additionally, fine particulate matter from industry, transport, and forest fires has been linked to prevalence of CKD [32].
Vulnerable populations bear the brunt of these risks, often living in inadequately protected environments, with limited access to cooling, greenery, and safe working conditions.
In 2024, the 77th World Health Assembly adopted a landmark Resolution on Climate Change and Health, recognizing the environmental crisis as a major threat to human well-being and calling for climate-resilient, low-carbon health systems. The Resolution pressed Member States to incorporate health into national climate strategies and endorsed mechanisms, such as the Alliance for Transformative Action on Climate and Health, to support implementation [33].
Building on this momentum, the 78th Resolution specifically emphasized coordinated global action on environmental threats to overall and kidney health. Together, these Resolutions create a compelling dual mandate: to place kidney health at the intersection of noncommunicable disease control and environmental stewardship, and to guide Member States toward more integrated, equitable, and sustainable health responses.
Addressing environmental risks, however, must go hand in hand with reducing the ecological footprint of kidney care itself (see below).
| Ecofriendly Kidney Failure Care: Toward Greener Nephrology | ▴Top |
The ideal approach to forestall the negative impact of interventions is taking measures, ensuring that they are no longer needed. Accordingly, prevention of kidney disease supports planetary sustainability by delaying or avoiding dialysis or reducing the use of pharmaceuticals, the production of which also has an environmental footprint. However, if drugs delay the progression of CKD and the need for kidney replacement therapy (KRT), this may compensate for the carbon footprint of drug production. A real-data secondary analysis of the placebo-controlled CREDENCE study, investigating the impact of canaglifozin on outcomes, found a 20% to 25% greenhouse gas reduction during 2.6 years of follow-up in patients with type 2 diabetes not yet on KRT [34, 35].
| Transplantation: Advancing Access and Sustainability | ▴Top |
Among KRTs, transplantation offers the best outcomes—lower societal costs, improved survival, enhanced quality of life, and significantly less environmental impact compared with dialysis [36, 37].
Yet, access to kidney transplantation varies widely across and within countries, influenced by health care infrastructure, socioeconomic status, and geography (rural vs. urban) [4]. Donation practices also differ: some countries rely heavily on living donors, whereas others focus mainly on deceased donation. In many areas, donation after cardiac death or preemptive transplantation remains underutilized, despite favorable outcomes [38, 39]. Furthermore, potential donors and recipients are frequently disqualified on the basis of arbitrary criteria or prejudices, with the exclusion of specific social groups, age categories, women, individuals with nonessential comorbidities, or borderline donors. Excluding borderline donors also reduces the donor pool, despite evidence that kidneys from borderline donors are safe, provided careful assessment, long-term follow-up, and treatment of risk factors [40]. In low-resource settings, kidney transplantation programs are often underdeveloped or absent, further deepening health inequities and enhancing economic burden.
Reducing transplantation disparities requires clear, globally endorsed guidelines on program design, ethical and legal frameworks on how to react to paid donation, and both technical and institutional support from countries or units with advanced transplantation programs. Efforts should also include public education programs to expand the donor pool, and to address cultural, religious, and societal concerns.
| Sustainable Dialysis: Reducing Environmental Impact While Improving Access | ▴Top |
Most people on KRT receive dialysis despite the many disadvantages mentioned above [37, 41]. In recent years, the environmental burden of dialysis has emerged as an added concern.
The health care sector heavily impacts environmental degradation [42]. Dialysis is one of the main contributors, because of its repetitive and long-lasting water and energy consumption, greenhouse gas emission, and plastic waste generation [6]. Although therapeutic activities are a direct part of this process, approximately 70% of health care–related greenhouse gas emissions stem from the supply chain, largely related to manufacturing, transport, and waste handling [6, 43, 44]. In addition, substantial volumes of spent dialysate and reverse osmosis reject are usually discarded through the drain system, a particular issue in arid regions or during droughts [6, 45].
Urgent action is needed: investment in ecofriendly dialysis technologies, which must prioritize patient safety by reducing toxicity from microplastics and eluates, while also improving the treatment experience by addressing stressors, like excessively noisy machines; critical review of the clinical procedures to reduce environmental footprint without affecting treatment quality; and greater transparency about the burdens of manufacturing and transport and how they are addressed (Fig. 2) [6]. This responsibility requires collaboration among industry, physicians, patients, nurses, engineers, chemists, and environmental scientists.
Home-based therapies—peritoneal dialysis and most home hemodialysis regimens, except daily extended dialysis—offer environmental advantages versus in-center hemodialysis, including reduced patient and personnel transportation needs, lower energy consumption for room temperature control, lower reverse osmosis plant electricity consumption, and, with compact hemodialysis systems and peritoneal dialysis, less water consumption. Peritoneal dialysis has a smaller footprint than in-center hemodialysis [43, 46, 47], even if transporting its bulkier supplies may still generate substantial emissions, particularly when transport distance is high [46]. Most home hemodialysis regimens are also suggested to show a benefit versus in-center hemodialysis, except for 6 × 8-h extended hemodialysis (300 mL/min dialysate flow) [47]. Incremental dialysis may further decrease environmental burden, together with dialysate flow optimization [48], if this is clinically suitable, and provided informed consent is obtained.
Peritoneal dialysis and existing compact hemodialysis systems can also help expand dialysis access in low-resource settings and in crises. In addition, several systems regenerating dialysate over sorbents are currently under development or undergoing preliminary clinical testing but are not yet available for widespread clinical use [49]. However, to achieve availability in emerging countries, barriers like import taxes or transport costs must be addressed (e.g., through local manufacturing).
| Comprehensive Conservative Care: Indispensable But Often Forgotten | ▴Top |
Comprehensive conservative or palliative care is the third option for treating kidney failure, next to transplantation and dialysis. This approach focuses on maximizing quality of life through full medical support, without initiating KRT [50].
Conservative care is particularly appropriate for frail and elderly people, many of whom show a rapid decline in functional status and increased mortality in the first year after dialysis start [51]. People with CKD stages 3 to 5 preferred conservative care if dialysis implied an increase in hospital visits or restricted travel capacity [52]. Despite this, conservative care often remains underutilized [50, 53].
Educational initiatives aimed at both people with kidney disease and health care professionals should increase awareness and understanding of conservative care. Promoting this approach more broadly can ensure people receive treatments aligned with their values, circumstances, and wishes, while reducing unnecessary medical, economic, and environmental burdens.
| Patient Empowerment: The Elephant in the Room | ▴Top |
Many people report that the information provided before starting KRT is of average to poor quality, particularly in countries with lower gross domestic product [54].
Paternalistic decision-making remains common, overlooking opportunities for early modality planning, vascular access creation, and elective KRT initiation. By contrast, shared decision-making actively engages patients in treatment choices, enhancing satisfaction, quality of life, outcomes, transplantation, and home dialysis rates, and reducing reliance on in-center hemodialysis [54, 55].
The current hospital structures remain highly patient unfriendly, making even vocal people poorly heard. Readily accessible smaller hospital-independent outpatient units, increased nurse involvement in consultations, and discussion groups with active patient participation are possible innovative options, next to several educational and informative initiatives elaborated throughout this text. Support by patient organizations could help to advance these evolutions.
Effective predialysis care, accurate risk prediction, and strategic modality planning are crucial for improving outcomes and reducing health care costs, but could be optimized, particularly in lower-resource areas, by forestalling late referral, fragmented care, inadequate patient education, poor adherence, and limited communication.
Patient involvement is also crucial in research design, data interpretation, and registry development, helping to steer efforts in directions that really matter to them. Patients also should be encouraged to participate in training programs that build confidence and communication skills, empowering them to become active care partners and shape the future of kidney health [56].
| Kidney Care in Crisis Situations: Adapting to a Changing World | ▴Top |
The number of people affected by crisis situations is steadily increasing, driven by population growth, climate change, and increasing geopolitical instability. These crises range from natural disasters (earthquakes, floods, extreme weather, and pandemics) to human-made emergencies, particularly armed conflicts [57].
People with kidney diseases are particularly vulnerable as they depend on specialized medication and resource-intensive treatments, like dialysis. These require skilled staff, clean water, electricity, functional machines, transport possibilities to supply stock, and reliable infrastructure—resources typically compromised in crises [57].
Missing dialyses can quickly lead to life-threatening complications, such as hyperkalemia, which may require urgent evacuation [58]. Interruption of drug therapies may accelerate CKD progression or cause kidney graft rejection. Despite these risks, people with kidney diseases are rarely considered in official disaster plans.
With crises becoming more frequent and severe, kidney health should be integrated in disaster planning and emergency protocols. Authorities should be made aware of the nephrological community’s specific needs through strong coordinated advocacy. In case of noninclusion of kidney care in general disaster plans, the nephrology communities and nephrologists should develop their own. Simultaneously, there is an urgent need for less resource-dependent treatment strategies.
| Call to Action: A Collective and Global Responsibility | ▴Top |
The traditional kidney care model aligned around in-center hemodialysis is no longer sustainable—ecologically, economically, and ethically (Fig. 1). People living with CKD urgently need better quality of life and care. Transformation requires a holistic approach (Table 1), with all stakeholders considering each of the key areas discussed above—adapted to local situations, infrastructure, and resources.
WKD 2026 amplifies this need, issuing a call to global action:
- The public should be educated to ask care providers about their kidney parameters and function.
- Workers, particularly those employed outdoors in agriculture and construction, should be sensitized about occupational threats of heat and environmental pollution and how to mitigate these to preserve kidney health.
- People with kidney disease and their communities should be empowered to take an active role in shaping care pathways that serve their needs to their benefit.
- Health care professionals must shift emphasis toward integrated, preventive, and community-based care that enhances well-being and environmental responsibility, with focus on early disease and out-of-hospital approaches.
- Researchers and industry must challenge the status quo and prioritize innovation, striving toward equity, flexibility, patient friendliness, and sustainability.
- Policy makers and administrators need to recognize the cardio-kidney-metabolic cluster as a critical public health threat, prompting system redesign, and promoting sustainable kidney care by funding and reimbursement initiatives.
- Patient advocacy organizations must be recognized as essential partners in design, implementation, and evaluation of policy initiatives to ensure the system is built around patient-specific needs. However, active advocacy is a responsibility of the entire kidney care community.
- Global health partnerships should link these efforts, advocating at all levels for cohesive future-ready kidney care and global health.
Widespread lack of awareness—among the public, policy makers, and even health professionals—contributes to persistent inequities across socioeconomic, gender (social or cultural rather than biological identity), ethnic, national, and regional lines. Tackling this requires robust education that highlights the public health threats and general burden imposed by kidney damage and kidney diseases.
Given the demographic and geopolitical trends, appropriate well-planned screening, early detection, and prevention are the first and foremost steps to reach sustainability goals. These measures reduce complications, progression to advanced kidney disease, and the need for KRT. Prevention will ultimately also favor global health by mitigating the course of diseases frequently causing or complicating CKD and/or accelerated by CKD, significantly decreasing personal and societal problems, which emerge already in robust social security systems. In the absence of universal coverage, this will have even more important benefits, by avoiding early fatal outcomes and devastating financial consequences for many.
| Conclusion: Aligning Kidney Health With Global Health and Sustainability Agendas | ▴Top |
The recognition of kidney diseases as a global priority by the World Health Organization at the 78th World Health Assembly marks a pivotal moment [5]. It provides a comprehensive mandate for urgent action and a strong foundation for national and international advocacy.
The 2026 WKD theme catalyzes the embedding of kidney health and care within broader health and sustainability. This shift to patient-centered models must be championed by all stakeholders who share this responsibility to realize this model, across health, environment, labor, and policy sectors, through partnership-aligned movements and coalitions with groups with parallel interests across organ specialties.
This publication and WKD 2026 issue an urgent, united call to prioritize kidney health as a pillar of a healthier, fairer, and more sustainable future. The decisions made now will determine the life of millions for decades to come.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
All the authors declared no competing interests.
Author Contributions
All authors have contributed equally to the preparation of this manuscript.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Francis A, Harhay MN, Ong ACM, Tummalapalli SL, Ortiz A, Fogo AB, Fliser D, et al. Chronic kidney disease and the global public health agenda: an international consensus. Nat Rev Nephrol. 2024;20(7):473-485.
doi pubmed - GBD 2023 Kidney Failure with Replacment Therapy Collaborators. Global, regional, and national prevalence of kidney failure with replacement therapy and associated aetiologies, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023. Lancet Glob Health. 2025;13(8):e1378-e1395.
doi pubmed - Vanholder R, Annemans L, Bello AK, Bikbov B, Gallego D, Gansevoort RT, Lameire N, et al. Fighting the unbearable lightness of neglecting kidney health: the decade of the kidney. Clin Kidney J. 2021;14(7):1719-1730.
doi pubmed - Vanholder R, Annemans L, Braks M, Brown EA, Pais P, Purnell TS, Sawhney S, et al. Inequities in kidney health and kidney care. Nat Rev Nephrol. 2023;19(11):694-708.
doi pubmed - World Health Organization. Reducing the burden of noncommunicable diseases through promotion of kidney health and strengthening prevention and control of kidney disease. Accessed January 12, 2026. https://apps.who.int/gb/ebwha/pdf_files/EB156/B156_(20)-en.pdf.
- Vanholder R, Agar J, Braks M, Gallego D, Gerritsen KGF, Harber M, Noruisiene E, et al. The European Green Deal and nephrology: a call for action by the European Kidney Health Alliance. Nephrol Dial Transplant. 2023;38(5):1080-1088.
doi pubmed - Vanholder R, Coppo R, Bos WJW, Damato E, Fakhouri F, Humphreys A, Nistor I, et al. A policy call to address rare kidney disease in health care plans. Clin J Am Soc Nephrol. 2023;18(11):1510-1518.
doi pubmed - Gregg EW. Diabetes-related disability as a target for prevention. Lancet Diabetes Endocrinol. 2013;1(2):81-82.
doi pubmed - Vanholder R, Annemans L, Brown E, Gansevoort R, Gout-Zwart JJ, Lameire N, Morton RL, et al. Reducing the costs of chronic kidney disease while delivering quality health care: a call to action. Nat Rev Nephrol. 2017;13(7):393-409.
doi pubmed - World Kidney Day. 8 golden rules animated visuals. Accessed January 12, 2026. https://www.worldkidneyday.org/facts/8-golden-rules/.
- Norton JM, Moxey-Mims MM, Eggers PW, Narva AS, Star RA, Kimmel PL, Rodgers GP. Social determinants of racial disparities in CKD. J Am Soc Nephrol. 2016;27(9):2576-2595.
doi pubmed - Ferro CJ, Wanner C, Luyckx V, Stevens K, Cerqueira S, Darwish R, Fernandez BF, et al. ABCDE to identify and prevent chronic kidney disease: a call to action. Nephrol Dial Transplant. 2025;40(9):1786-1798.
doi pubmed - Heerspink HJ, Desai M, Jardine M, Balis D, Meininger G, Perkovic V. Canagliflozin slows progression of renal function decline independently of glycemic effects. J Am Soc Nephrol. 2017;28(1):368-375.
doi pubmed - Cordero L, Ortiz A. Albuminuria-based universal screening for CKD should be implemented now in high-income countries. Kidney Int. 2025;108(5):754-759.
doi pubmed - Stehle T, Delanaye P. Which is the best glomerular filtration marker: Creatinine, cystatin C or both? Eur J Clin Invest. 2024;54(10):e14278.
doi pubmed - van Mil D, Kieneker LM, Evers-Roeten B, Thelen MHM, de Vries H, Hemmelder MH, Dorgelo A, et al. Participation rate and yield of two home-based screening methods to detect increased albuminuria in the general population in the Netherlands (THOMAS): a prospective, randomised, open-label implementation study. Lancet. 2023;402(10407):1052-1064.
doi pubmed - Tangri N, Alvarez CS, Arnold M, Barone S, Cebrian A, Chen H, De Nicola L, et al. Suboptimal monitoring and management in patients with unrecorded stage 3 chronic kidney disease in real-world settings: Insights from REVEAL-CKD. Eur J Clin Invest. 2024;54(11):e14282.
doi pubmed - Pouwels X, van Mil D, Kieneker LM, Boersma C, van Etten RW, Evers-Roeten B, Heerspink HJL, et al. Cost-effectiveness of home-based screening of the general population for albuminuria to prevent progression of cardiovascular and kidney disease. EClinicalMedicine. 2024;68:102414.
doi pubmed - Chavarina KK, Lou-Meda R, Luyckx VA. Strategic rebalancing of kidney-related investments is key to implementing the WHO kidney health resolution. Nat Rev Nephrol. 2025;21(12):813-814.
doi pubmed - Kidney Disease Screening and Awareness Program. Together we fight kidney disease. Accessed January 12, 2026. www.kdsap.org.
- Afkarian M, Sachs MC, Kestenbaum B, Hirsch IB, Tuttle KR, Himmelfarb J, de Boer IH. Kidney disease and increased mortality risk in type 2 diabetes. J Am Soc Nephrol. 2013;24(2):302-308.
doi pubmed - Wan EYF, Yu EYT, Chin WY, Fong DYT, Choi EPH, Tang EHM, Lam CLK. Burden of CKD and cardiovascular disease on life expectancy and health service utilization: a cohort study of Hong Kong Chinese hypertensive patients. J Am Soc Nephrol. 2019;30(10):1991-1999.
doi pubmed - Luyckx VA, Ulasi II. Kidney disease must be counted everywhere. Lancet. 2025;406(10518):2401-2403.
doi pubmed - Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2024;105(4S):S117-S314.
doi pubmed - Chinta RK, Shri V, Milojkovic B, Begos D, Kemisetti S, Chintagunti NK, Bikbov B, et al. Point-of-care testing and integrated digital health technology for CKD screening in high-risk populations of India. Kidney Int Rep. 2025;10(7):2128-2139.
doi pubmed - Guedes M, Dias PT, Rea RR, Calice-Silva V, Lopes M, Brandao AA, Bauer AC, et al. Patterns of kidney function and risk assessment in a nationwide laboratory database: the Brazilian CHECK-CKD study. BMC Nephrol. 2024;25(1):191.
doi pubmed - Hajat S, Casula A, Murage P, Omoyeni D, Gray T, Plummer Z, Steenkamp R, et al. Ambient heat and acute kidney injury: case-crossover analysis of 1 354 675 automated e-alert episodes linked to high-resolution climate data. Lancet Planet Health. 2024;8(3):e156-e162.
doi pubmed - Maline GE, Goldfarb DS. Climate change and kidney stones. Curr Opin Nephrol Hypertens. 2024;33(1):89-96.
doi pubmed - Gopalakrishnan N, Sudharshini S, Sakthirajan R, Dineshkumar T, Moses Lamech T, Somasundaram A, Jayalakshmi S, et al. CKDu-AGRI Study-a population-based cross-sectional study of chronic kidney disease and chronic kidney disease of unknown aetiology among agricultural workers in Tamil Nadu, India. Lancet Reg Health Southeast Asia. 2025;42:100683.
doi pubmed - Garcia-Trabanino RA. The human burden of Mesoamerican nephropathy: diagnosis and treatment in a complex web of socioeconomics, context, and stigma. Semin Nephrol. 2025;45(1-2):151601.
doi pubmed - Chretien JP, Anyamba A, Small J, Britch S, Sanchez JL, Halbach AC, Tucker C, et al. Global climate anomalies and potential infectious disease risks: 2014-2015. PLoS Curr. 2015;7.
doi pubmed - Bowe B, Artimovich E, Xie Y, Yan Y, Cai M, Al-Aly Z. The global and national burden of chronic kidney disease attributable to ambient fine particulate matter air pollution: a modelling study. BMJ Glob Health. 2020;5(3):e002063.
doi pubmed - World Meteorological Organization, World Health Organization. Alliance for Transformative Action on Climate and Health (ATACH) meeting on accessing climate finance for health. Accessed January 12, 2026. https://climahealth.info/alliance-for-transformative-action-on-climate-and-health-atach-meeting-on-accessing-climate-finance-for-health/.
- Talbot B, Fletcher RA, Neal B, Oshima M, Adshead F, Moore K, McGain F, et al. The potential for reducing greenhouse gas emissions through disease prevention: a secondary analysis of data from the CREDENCE trial. Lancet Planet Health. 2024;8(12):e1055-e1064.
doi pubmed - Evaluation of the effects of canagliflozin on renal and cardiovascular outcomes in participants with diabetic nephropathy (CREDENCE). ClinicalTrials.gov identifier: NCT02065791. Updated December 5, 2019. https://clinicaltrials.gov/study/NCT02065791.
- Vanholder R, Dominguez-Gil B, Busic M, Cortez-Pinto H, Craig JC, Jager KJ, Mahillo B, et al. Organ donation and transplantation: a multi-stakeholder call to action. Nat Rev Nephrol. 2021;17(8):554-568.
doi pubmed - Tonelli M, Wiebe N, Knoll G, Bello A, Browne S, Jadhav D, Klarenbach S, et al. Systematic review: kidney transplantation compared with dialysis in clinically relevant outcomes. Am J Transplant. 2011;11(10):2093-2109.
doi pubmed - Schaapherder A, Wijermars LGM, de Vries DK, de Vries APJ, Bemelman FJ, van de Wetering J, van Zuilen AD, et al. Equivalent long-term transplantation outcomes for kidneys donated after brain death and cardiac death: conclusions from a nationwide evaluation. EClinicalMedicine. 2018;4-5:25-31.
doi pubmed - Azegami T, Kounoue N, Sofue T, Yazawa M, Tsujita M, Masutani K, Kataoka Y, et al. Efficacy of pre-emptive kidney transplantation for adults with end-stage kidney disease: a systematic review and meta-analysis. Ren Fail. 2023;45(1):2169618.
doi pubmed - Achkar KA, Abdelnour LM, Abu Jawdeh BG, Tantisattamoa E, Al Ammary F. Evaluation and long-term follow-up of living kidney donors. Adv Kidney Dis Health. 2024;31(5):400-407.
doi pubmed - Barraclough KA, Agar JWM. Green nephrology. Nat Rev Nephrol. 2020;16(5):257-268.
doi pubmed - Lenzen M, Malik A, Li M, Fry J, Weisz H, Pichler PP, Chaves LSM, et al. The environmental footprint of health care: a global assessment. Lancet Planet Health. 2020;4(7):e271-e279.
doi pubmed - Connor A, Lillywhite R, Cooke MW. The carbon footprint of a renal service in the United Kingdom. QJM. 2010;103(12):965-975.
doi pubmed - Piccoli GB, Nazha M, Ferraresi M, Vigotti FN, Pereno A, Barbero S. Eco-dialysis: the financial and ecological costs of dialysis waste products: is a 'cradle-to-cradle' model feasible for planet-friendly haemodialysis waste management? Nephrol Dial Transplant. 2015;30(6):1018-1027.
doi pubmed - Tarrass F, Benjelloun M, Benjelloun O. Recycling wastewater after hemodialysis: an environmental analysis for alternative water sources in arid regions. Am J Kidney Dis. 2008;52(1):154-158.
doi pubmed - McAlister S, Talbot B, Knight J, Blair S, McGain F, McDonald S, Nelson C, et al. The carbon footprint of peritoneal dialysis in Australia. J Am Soc Nephrol. 2024;35(8):1095-1103.
doi pubmed - Barraclough KA, Talbot B, Knight J, Blair S, McGain F, Masterson R, Knight R, et al. Carbon emissions from different dialysis modalities: a life cycle assessment. Am J Kidney Dis. 2025;86(4):465-474.e461.
doi pubmed - Solomon D, Arumugam V, Sakthirajan R, Lamech TM, Dineshkumar T, Vathsalyan P, Senthilkumaran G, et al. A pilot study on the safety and adequacy of a novel ecofriendly hemodialysis prescription-green nephrology. Kidney Int Rep. 2024;9(5):1496-1503.
doi pubmed - Ramada DL, de Vries J, Vollenbroek J, Noor N, Ter Beek O, Mihaila SM, Wieringa F, et al. Portable, wearable and implantable artificial kidney systems: needs, opportunities and challenges. Nat Rev Nephrol. 2023;19(8):481-490.
doi pubmed - Lunney M, Bello AK, Levin A, Tam-Tham H, Thomas C, Osman MA, Ye F, et al. Availability, accessibility, and quality of conservative kidney management worldwide. Clin J Am Soc Nephrol. 2020;16(1):79-87.
doi pubmed - Kurella Tamura M, Covinsky KE, Chertow GM, Yaffe K, Landefeld CS, McCulloch CE. Functional status of elderly adults before and after initiation of dialysis. N Engl J Med. 2009;361(16):1539-1547.
doi pubmed - Morton RL, Snelling P, Webster AC, Rose J, Masterson R, Johnson DW, Howard K. Factors influencing patient choice of dialysis versus conservative care to treat end-stage kidney disease. CMAJ. 2012;184(5):E277-283.
doi pubmed - Stel VS, de Jong RW, Kramer A, Andrusev AM, Baltar JM, Barbullushi M, Bell S, et al. Supplemented ERA-EDTA Registry data evaluated the frequency of dialysis, kidney transplantation, and comprehensive conservative management for patients with kidney failure in Europe. Kidney Int. 2021;100(1):182-195.
doi pubmed - de Jong RW, Stel VS, Rahmel A, Murphy M, Vanholder RC, Massy ZA, Jager KJ. Patient-reported factors influencing the choice of their kidney replacement treatment modality. Nephrol Dial Transplant. 2022;37(3):477-488.
doi pubmed - Joosten EA, DeFuentes-Merillas L, de Weert GH, Sensky T, van der Staak CP, de Jong CA. Systematic review of the effects of shared decision-making on patient satisfaction, treatment adherence and health status. Psychother Psychosom. 2008;77(4):219-226.
doi pubmed - European Patients Academy on Therapeutic Innovation (EUPATI). Education that empowers. Accessed January 12, 2026. https://eupati.eu/.
- Sever MS, Luyckx V, Tonelli M, Kazancioglu R, Rodgers D, Gallego D, Tuglular S, et al. Disasters and kidney care: pitfalls and solutions. Nat Rev Nephrol. 2023;19(10):672-686.
doi pubmed - Pawlowicz-Szlarska E, Vanholder R, Sever MS, Tuglular S, Luyckx V, Eckardt KU, Gallego D, et al. Distribution, preparedness and management of Ukrainian adult refugees on dialysis-an international survey by the Renal Disaster Relief Task Force of the European Renal Association. Nephrol Dial Transplant. 2023;38(10):2407-2415.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
World Journal of Nephrology and Urology is published by Elmer Press Inc.