| World Journal of Nephrology and Urology, ISSN 1927-1239 print, 1927-1247 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Nephrol Urol and Elmer Press Inc |
| Journal website https://wjnu.elmerpub.com |
Case Report
Volume 15, Number 3, July 2026, pages 90-93

Atraumatic Bilateral Page Kidney Treated With Laparoscopic Capsulectomy
Qi Yang Lima, b, Chloe Onga, Ho Yee Tionga, Wei Jin Chuaa
aDepartment of Urology, National University Hospital, Singapore
bCorresponding Author: Qi Yang Lim, Department of Urology, National University Hospital, Singapore
Manuscript submitted March 25, 2026, accepted April 6, 2026, published online July 8, 2026
Short title: Page Kidney Treated With Laparoscopic Capsulectomy
doi: https://doi.org/10.14740/wjnu1051
| Abstract | ▴Top |
Page kidney refers to external compression of the renal parenchyma, typically due to a subcapsular or perinephric collection, leading to hypertension through activation of the renin–angiotensin–aldosterone system (RAAS). Although most cases occur following trauma or iatrogenic injury, spontaneous bilateral Page kidney is possible but extremely rare. We report the case of a 22-year-old male rugby player who presented with left hypochondrial and epigastric pain. Initial computed tomography demonstrated bilateral perinephric hematomas without evidence of renal rupture. Renal function was preserved, but the patient subsequently developed persistent hypertension. Imaging revealed bilateral perinephric collections causing significant renal compression with elevated resistive indices. Initial management included angiotensin receptor blockade and ultrasound-guided percutaneous drainage. However, fluid collections recurred, resulting in persistent renal compression and hypertension. The patient therefore underwent staged laparoscopic resection of the renal capsule. Intraoperatively, decompression of the kidneys resulted in visible improvement in renal perfusion and size. Postoperatively, blood pressure control improved with medical therapy. Bilateral Page kidney is a rare but potentially reversible cause of secondary hypertension. Early recognition is crucial. While medical management and percutaneous drainage may be effective in selected cases, recurrent collections may require definitive surgical decompression. Laparoscopic capsulectomy represents a safe and effective treatment option in refractory cases.
Keywords: Page kidney; Secondary hypertension; Subcapsular hematoma; Laparoscopic capsulectomy; Renal compression
| Introduction | ▴Top |
The Page kidney phenomenon refers to extrinsic compression of the renal parenchyma, most commonly caused by a subcapsular or perirenal collection, leading to hypertension due to activation of the renin–angiotensin–aldosterone system (RAAS) secondary to renal hypoperfusion and microvascular ischemia [1–3].
In some cases, direct compression of major renal vessels may also contribute to renovascular hypertension [3].
Page kidney is an uncommon cause of secondary hypertension and is therefore often overlooked in clinical practice [4, 5]. However, it remains an important diagnosis because it represents a potentially reversible cause of hypertension [5].
Most reported cases occur following blunt trauma, renal biopsy, or other urological procedures [1–3, 6–9]. Spontaneous cases are rare and have been associated with conditions such as renal tumors, arteriovenous malformations, cyst rupture, urinomas, lymphatic cysts, inflammatory diseases, or anticoagulation therapy [2, 10–14].
We present a rare case of atraumatic bilateral Page kidney in a young patient with recurrent subcapsular collections requiring staged laparoscopic capsulectomy.
| Case Report | ▴Top |
A 22-year-old male university rugby player presented to the emergency department with left hypochondrial and epigastric pain. He reported no history of trauma prior to presentation. At presentation, his blood pressure was within normal limits.
A contrast-enhanced computed tomography (CT) scan of the abdomen and pelvis demonstrated bilateral perinephric hematomas with mild compression of both kidneys (Fig. 1). There was no evidence of renal rupture or vascular injury, and renal function was preserved. The initial working diagnosis, based on his presentation, sporting activities, and CT findings, was bilateral perinephric hematoma, likely related to minor trauma sustained during sporting activity.
 Click for large image | Figure 1. Coronal and axial computed tomography (CT) images demonstrating bilateral fluid-density perinephric collections causing mild compression of the renal parenchyma. |
The patient was initially managed conservatively with outpatient follow-up. During subsequent clinic visits, however, he was noted to have persistent hypertension, with systolic blood pressures ranging from 140 to 160 mm Hg and diastolic pressures between 90 and 110 mm Hg.
Further evaluation for secondary hypertension was performed. Repeat imaging with renal ultrasound revealed persistent bilateral perinephric collections exerting significant mass effect on the kidneys. Doppler studies demonstrated elevated peak systolic velocities and increased resistive indices, suggesting renal compression.
The patient was started on telmisartan 40 mg once daily only and subsequently underwent ultrasound-guided percutaneous drainage of the bilateral perinephric collections (Fig. 2). Fluid analysis demonstrated urea and creatinine concentrations similar to serum levels, with no triglycerides detected. Based on these findings, the working diagnosis was bilateral renal seroma.
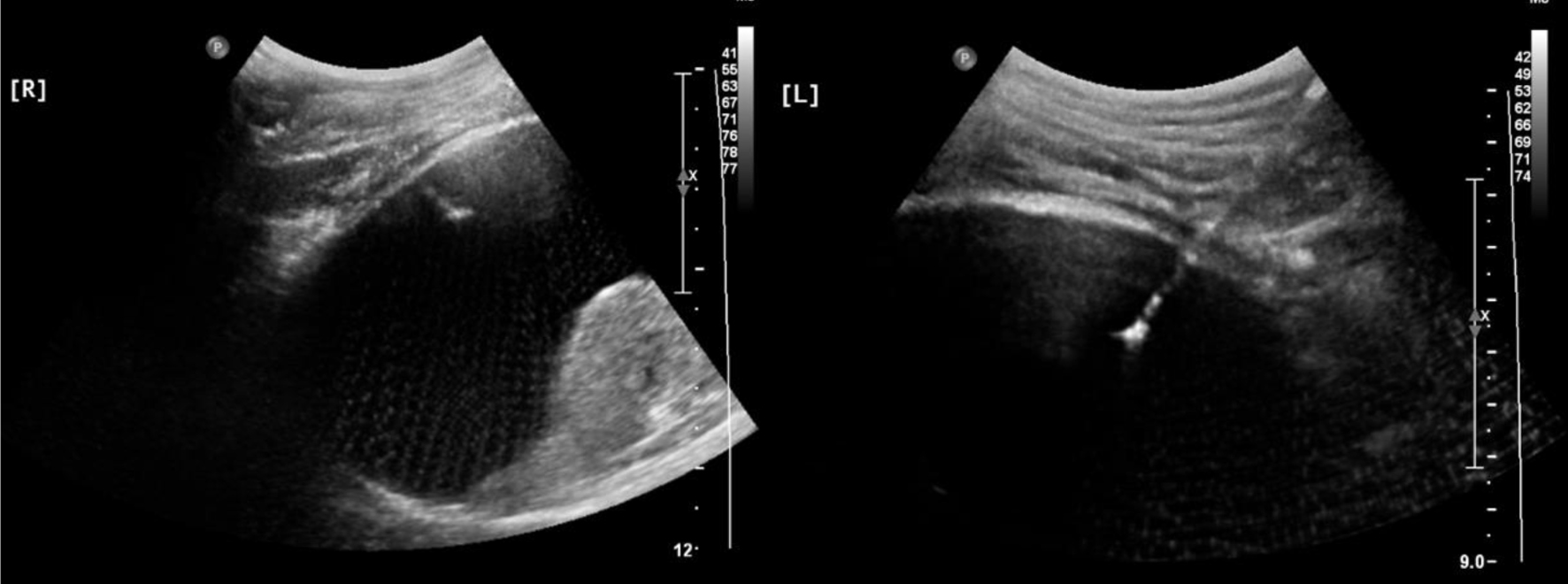 Click for large image | Figure 2. Ultrasound-guided needle aspiration and drain insertion of bilateral perirenal collections. |
Despite drainage, follow-up ultrasound demonstrated re-accumulation of the perinephric fluid collections.
A repeat CT scan confirmed persistent bilateral subcapsular fluid collections with significant mass effect on both kidneys and focal narrowing of the left renal vein (Fig. 3). The patient’s blood pressure temporarily improved following drainage, with systolic blood pressure ranging from 120 to 130 mm Hg and diastolic pressures between 70 and 80 mm Hg, allowing discontinuation of telmisartan.
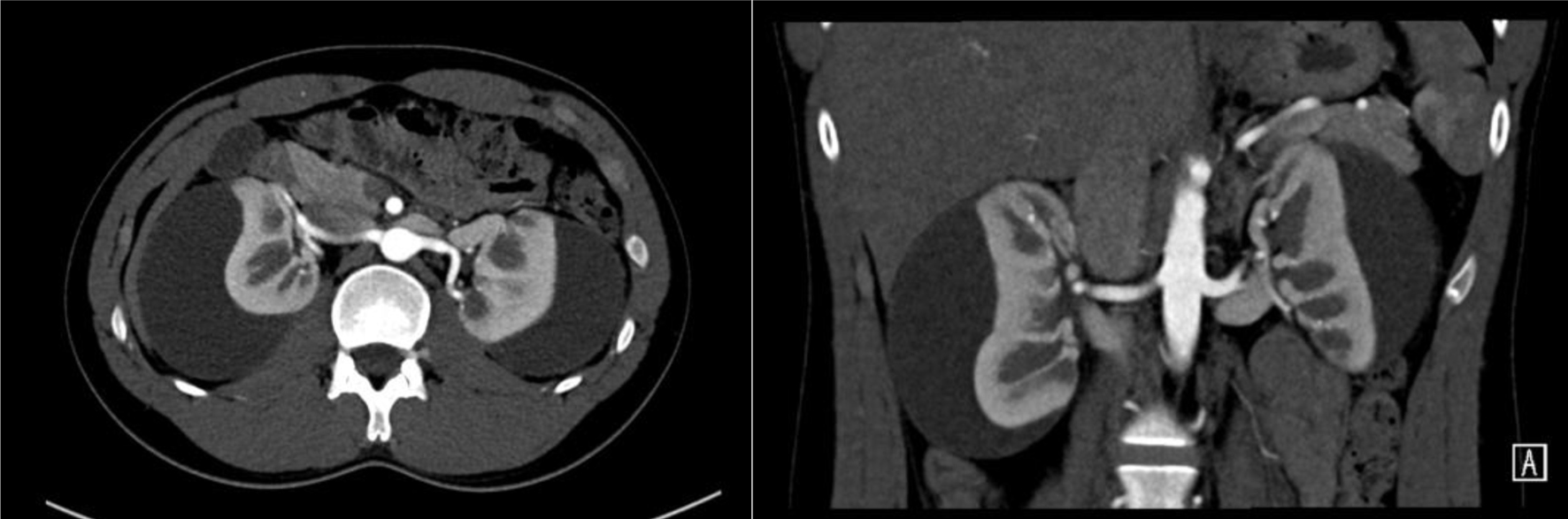 Click for large image | Figure 3. Contrast computed tomography (CT) demonstrating bilateral subcapsular fluid collections with renal compression and narrowing of the left renal vein. |
Given persistent compression, the patient underwent laparoscopic resection of the right renal capsule. Histopathological examination demonstrated fibrous capsule with mild patchy chronic inflammation.
Although the patient initially recovered well, follow-up imaging revealed re-accumulation of small amount of right-sided perinephric fluid, while the left-sided collection remained stable. As the patient’s hypertension recurred, telmisartan was restarted at the same dose of 40 mg once daily.
Subsequent CT imaging demonstrated progression of the left-sided collection, and the patient therefore underwent laparoscopic resection of the left renal capsule.
Intraoperatively, clear straw-colored fluid was drained from both kidneys, consistent with the revised working diagnosis of seroma. Following decompression and capsulectomy, the kidneys—initially small and pale—visibly increased in size and perfusion, suggesting immediate restoration of renal blood flow (Fig. 4). Subsequently, the patient’s blood pressure returned to normal, with systolic values ranging from 120 to 130 mm Hg and diastolic values from 70 to 80 mm Hg, allowing discontinuation of telmisartan.
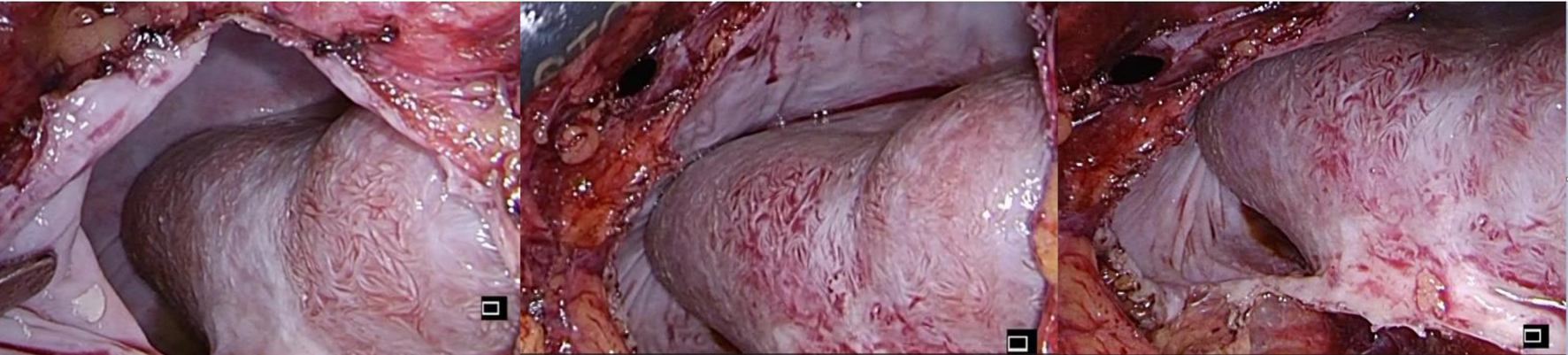 Click for large image | Figure 4. Intraoperative images demonstrating decompression of the kidney following laparoscopic capsulectomy with restoration of renal perfusion. |
| Discussion | ▴Top |
The Page kidney phenomenon was first described by Irving Page in 1939 [15], who demonstrated experimental hypertension in animal models by wrapping kidneys in cellophane to induce compression. The first clinical case was reported in 1955, describing hypertension secondary to a subcapsular hematoma [16].
The pathophysiology of Page kidney is primarily related to renal ischemia and hypoperfusion caused by compression of the renal parenchyma [1–3]. This activates the RAAS, resulting in sodium retention, volume expansion, and hypertension. Additionally, direct compression or stenosis of major renal vessels may further contribute to renovascular hypertension.
Page kidney has been reported across all age groups. The most common etiologies include blunt renal trauma, iatrogenic causes such as renal biopsy or urological procedures, anticoagulation-related spontaneous hemorrhage, renal tumors or vascular malformations, and inflammatory conditions [1–3, 6–9, 11–14].
Management strategies depend on the severity of renal compression, renal function, and necessary blood pressure control.
Conservative management may be appropriate in patients with minimal compression and stable renal function [5, 17]. This typically involves blood pressure control with RAAS-targeted therapy, such as angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers.
For patients with significant collections, percutaneous drainage may relieve renal compression, improve renal perfusion and hypertension may be delayed [18, 19]. However, recurrence of the collection is not uncommon, particularly when the capsule has become fibrotic.
In such cases, surgical decompression becomes necessary [19, 20]. Both open and laparoscopic approaches have been described. Laparoscopic capsulectomy allows effective decompression while minimizing surgical morbidity.
Conclusions
Bilateral Page kidney is a rare but important cause of secondary hypertension. Early recognition and appropriate imaging are essential for diagnosis. Although medical therapy and percutaneous drainage may be effective in selected cases, recurrent collections may require surgical decompression. Laparoscopic renal capsulectomy represents a safe and effective definitive treatment in patients with persistent renal compression and recurrent fluid collections.
Learning points
Our case illustrates several important clinical points: Bilateral Page kidney is extremely rare. Hypertension may develop delayed after the initial insult. Percutaneous drainage may not be definitive. Laparoscopic capsulectomy provides durable decompression.
Acknowledgments
The authors would like to thank the National University Hospital, Singapore, for their support in the management of this case.
Financial Disclosure
The authors declare that no funding was received for this study.
Conflict of Interest
The authors declare no conflict of interest.
Informed Consent
Informed consent was obtained from the patient for publication of this case report and accompanying images.
Author Contributions
Qi Yang Lim: conceptualization, data collection, and manuscript drafting. Chloe Ong: data collection and literature review. Ho Yee Tiong: supervision and critical revision of manuscript. Wei Jin Chua: supervision and final approval of manuscript.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- McCune TR, Stone WJ, Breyer JA. Page kidney: case report and review of the literature. Am J Kidney Dis. 1991;18(5):593-599.
doi pubmed - Kenis I, Werner M, Nacasch N, Korzets Z. Recurrent non-traumatic page kidney. Isr Med Assoc J. 2012;14(7):452-453.
pubmed - Diamond JA. Hypertension due to perinephric compression: the "Page" kidney. Am J Hypertens. 2001;14(3):305.
doi pubmed - Smyth A, Collins CS, Thorsteinsdottir B, Madsen BE, Oliveira GH, Kane G, Garovic VD. Page kidney: etiology, renal function outcomes and risk for future hypertension. J Clin Hypertens (Greenwich). 2012;14(4):216-221.
doi pubmed - Dopson SJ, Jayakumar S, Velez JC. Page kidney as a rare cause of hypertension: case report and review of the literature. Am J Kidney Dis. 2009;54(2):334-339.
doi pubmed - John J, Allen S, Perry M, Patel HR, O'Brien T. Page kidney phenomenon presenting as acute renal failure after partial nephrectomy: a case report and review of the literature. Urol Int. 2008;80(4):440-443.
doi pubmed - Sasaguri M, Noda K, Matsumoto T, Shirai K, Tsuji E, Tsuji Y, Arakawa K. A case of hyperreninemic hypertension after extracorporeal shock-wave lithotripsy. Hypertens Res. 2000;23(6):709-712.
doi pubmed - Mufarrij P, Sandhu JS, Coll DM, Vaughan ED, Jr. Page kidney as a complication of percutaneous antegrade endopyelotomy. Urology. 2005;65(3):592.
doi pubmed - Kamar N, Sallusto F, Rostaing L. Acute Page kidney after a kidney allograft biopsy: successful outcome from observation and medical treatment. Transplantation. 2009;87(3):453-454.
doi pubmed - Warnich I, Nicolaou M, Sofianos Z, Pienaar JA, Varghese J. Page kidney: a rare cause of secondary hypertension. SA J Radiol. 2019;23(1):1762.
doi pubmed - Hurley PR, Kark AE. Bilateral subcapsular hematoma of the kidney. A complication of anticoagulant therapy. Br J Urol. 1973;45(4):342-344.
- Gillies MA, Maxwell SR, Watson AC. Spontaneous bilateral subcapsular renal haematomas associated with warfarin therapy. Scott Med J. 2003;48(3):72-73.
- Moorthy AV, Venugopal S, David S. Bilateral subcapsular hematomas after renal biopsy. Clin Nephrol. 1981;16(3):143-145.
- Shih CW, Wu MJ, Sung JM, et al. Bilateral subcapsular hematoma and perirenal abscess in a patient with polycystic kidney disease. Kidney Int. 2003;63(1):154-157.
- Page IH. The production of persistent arterial hypertension by cellophane perinephritis. JAMA. 1939;113:2046-2048.
- Engel WJ, Page IH. Hypertension due to renal compression resulting from subcapsular hematoma. J Urol. 1955;73(5):735-739.
doi pubmed - Myrianthefs P, Aravosita P, Tokta R, Louizou L, Boutzouka E, Baltopoulos G. Resolution of Page kidney-related hypertension with medical therapy: a case report. Heart Lung. 2007;36(5):377-379.
doi pubmed - Suckling R, Uddin F, Pilcher J, MacPhee IA, Eastwood JB, Banerjee D. Page kidney: successful radiological management of acute renal failure. Nephrol Dial Transplant. 2006;21(6):1740.
doi pubmed - Ciftci S, Stuart Wolf J, Jr. Laparoscopic treatment of Page kidney: a report of two cases and review of the literature. Turk J Urol. 2013;39(2):126-130.
doi pubmed - Vallina VL, Velasco JM, McDonald JC. Laparoscopic management of subcapsular and perinephric hematomas. Surg Endosc. 1997;11(3):272-275.
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
World Journal of Nephrology and Urology is published by Elmer Press Inc.